Complications of mastoiditis
•Descargar como PPTX, PDF•
31 recomendaciones•16,408 vistas

summary of complications of mastoiditis. presented in academic meeting at ELHC, SA

Recomendados
Más contenido relacionado
La actualidad más candente
La actualidad más candente (20)
Destacado
Destacado (20)
Similar a Complications of mastoiditis
Similar a Complications of mastoiditis (20)
Más de sarita pandey
Más de sarita pandey (12)
Último
Último (20)
Complications of mastoiditis
- 1. Complications of mastoiditis Sarita pandey
- 2. introduction • Mastoid process is an inferior extension of the petrous temporal bone • Provides a structural function as an anchor point for large muscles of the neck • Contains multiple air cells that develop from single main cavity (antrum) • In X section is has a honey comb appearance
- 3. Mastoid process • Sternocleidomastoid • Splenius capitus • Posterior belly of digastric • Longissimus capitus muscle
- 4. introduction • Tympanic cavity of middle ear is in communication with the mastoid antrum via aditus • Mastoid air cells are related superiorly to middle cranial fossa and posteriorly to posterior cranial fossa • Acute mastoiditis is serious complication of acute OM • Mastoiditis occurs when supperative infection extends from middle ear affected by OM to mastoid air cells • Once mastoiditis sets in it in it self has more complications.
- 5. Classification of mastoiditis • Classic or acute Mastoiditis – complication of AOM • Chronic, latent or masked mastoiditis presents in chronic or subclinical fashion • Associated with CSOM or Cholesteatoma
- 6. Epidemiology • Acute mastoiditis prior to advent of antibiotics was common • Developed in 5 – 10% of children with AOM • Mortality rate 2/100000 children • Currently 0.12/1000 child per year • Mortality rate < 0.01/100000 • Estimated that In every 50000 child with AOM 1 child develops mastoiditis
- 7. Acute mastoiditis • Much more common in young children with peak incidence at 6 – 13 months • Immunocompromised patients more prone to mastoiditis • Children/adults with intellectual impairment or communication difficulties thought to be susceptible to mastoiditis • Pre-existence of cholesteatoma is a known risk factor
- 8. Infecting organisms • Streptococcus pneumonia 25% prevalence • H Influenza • S. pyognes • Staphyloccus spp • Pseudomonas aeruginosa (becoming more common as widespread use of Abs increases) • Moraxella Catarrahalis • Gm neg bact • Mycobacteria • Aspergillus & other fungi (immunocompromised patients)
- 9. Presentation - acute mastoiditis • History of acute or recurrent episodes of OM • Otalgia or pain behind ear • Fever • Swelling, redness or boggy, tender mass post auricular region • Irritable infant, with feeding difficulties • Forward protrusion of external ear, may have fluctuance in the mass • Ear discharge/ middle ear effusion •
- 10. Presentation – chronic mastoiditis • Presents in a subtle or subclinical fashion after an episode of AOM • Recurrent bouts of otalgia and retro- aural pain • Recurrent headaches • Febrile episodes • TM may appear infected or postero-superior retraction/ perforation with pus • May be no external evidence of peri mastoid inflammation
- 11. Investigations: • FBC – leucocytosis • Elevated ESR • Blood cultures • Pus swab of any pus/ fluid in middle ear • CT gold standard • IF intracranial spread suspected LP • Audiogram once pain under control.
- 12. Management • Manage as an IN patient • To prevent likelihood of complications • High dose broad spectrum iv antibiotics for at least 48 hours • Oral antibiotics may be used after 48 hours if clinically improving • Anti pyretic • Myringotomy plus grommet as therapeutic and diagnostic procedure
- 13. Surgical management • Mastoidectomy • Mastoid osteitis • Co –existing cholesteatoma • Limited improvement after ivi meds
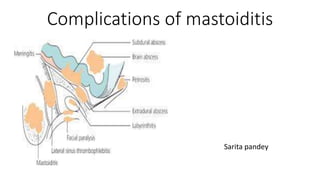
- 14. Complications of mastoiditis • Rare due to prompt antibiotic treatment, however with emergence of resistant organisms – may be higher in future • Clinically divided into: • Intratemporal • Intracranial • Systemic • cervical
- 15. Extension of infection… • Direct extension through the de-mineralized bone seen in cholesteatoma • Haematogenous spread via the veins, through bone and dura to the venous sinuses. • Through round or oval window into the auditory meatus on the vestibular aqueducts • Dehiscence of bony covering over the jugular bulb or the tegmen tympani • Neoplastic or accidental bony erosion • Through surgical defects in post stapedectomy surgery.
- 16. Intra - temporal • Coalescent Mastoiditis • When mastoid region inflammation cannot be arrested • Suppuration under pressure causes local acidosis and osseous decalcification, ischaemia and osteoclastic dissolution of the pneumatic cell walls • These cells can coalesce into larger cavities filled with purulent exudates and granulations • Resulting in empyema & coalescent mastoiditis • Antonelli et al – concluded that erosion of the cortical plate overlying the sigmoid sinus was the most sensitive and specific CT scan finding for distinguishing coalescent vs incipient acute mastoiditis
- 17. Coalescent mastoiditis • Spread of the inflammatory debris anteriorly to middle ear via aditus ad antrum can result in spontaneous resolution if the TM is perforated • Infection may spread laterally and produce sub periosteal abscess • May spread medially to petrous air cells, causing petrositis • Coalescent mastoiditis is diagnosed when CT demonstrates erosion of mastoid septa or mastoid walls
- 18. Coalescent mastoiditis • Latent mastoiditis (subclinical and often “masked”) • Indolent temporal bone infection with few clinical symptoms • Often owing to previous usage of broad spectrum antibiotic to treat Middle ear disease • TM is intact and middle ear shows no abnormalities at otoscopy • Disease progresses silently until an intracranial complication such as venous Dural thrombosis occurs • CT diagnostic, demonstrates the temporal bone disease and the intracranial complication
- 19. Sub periosteal abscess • Decalcification of the outer mastoid cortical bone results in abscess that can extend towards • Ext auditory canal • Spread along the zygomatic bone • Post auricular region
- 20. Perisinus abscess • When osteolysis occurs in the internal mastoid cortex • Direct apposition of the inflammatory debris to dura over the sigmoid sinus • Resulting in formation of perisinus and epidural abscess
- 21. Petrositis • Petrositis or petrous apicitis – rare complication that theoretically occurs only in individuals with pneumatized petrous apex • Patient present with CN VI palsy, deep facial pain and ipsilateral otorrhoea ( Gradenigo syndrome) • Facial pain due to focal meningitis over the petrous apex with irritation of the gasserian ganglion in the Meckel cave • Abducens nerve involvement occurs at its course through the Dorello canal • CT demonstrates erosive changes of the petrous apex with abn enhancement of adjacent meningitis
- 23. Other intratemporal complications • Labyrinthitis • CN VII palsy • SNHL • More common in chronic otitis media with cholesteatoma • Infection can spread into the labyrinth via the round or oval window or by direct invasion of the bony labyrinth • May result in suppurative labyrinthitis • Suspect when patient with infected ear develops sudden vertigo, nystagmus and hearing loss
- 24. Intracranial complications • Epidural abscess • Most common intracranial complication • Results from spread by contiguity following bone destruction in coalescent mastoiditis • Can occur in middle cranial fossa • Posterior cranial fossa is more common • Due to osseous destruction in the Trautmann triangle over the sigmoid sinus plate or in the posterior cortex of petrous pyramid • CT is mandatory for Diagnosis
- 25. Dural venous thrombophlebitis • As an result form extradural abscess • Sigmoid sinus thrombosis as a protective mechanism in attempt to localise infection • Thrombus may cause propagation to jugular vein, to other sinuses • Through emissary veins to subcutaneous tissue • Diagnosis may be difficult to make on basis of clinical picture alone • May be completely asymptomatic • Present as sign of toxaemia, intracranial hpt or hydrocephalus • Mastoidectomy with surgical exposure of the dura and removal of the granulation tissue • Use of anticoagulation and ligation of IJV are controversial
- 27. Subdural empyema • Several veins and veinules in middle normally communicate through intact bone and dura with vessels in subarachnoid space and brain parenchyma • Spread of infection and microorganisms through these veins reach subdural and subarachnoid space • Develops in interhemispheric fissure and along the tentorium cerebelli • CT = widening of the extra cerebral space with compression of adjacent sulci • Loculations within collection common
- 28. subdural
- 29. Other intracranial complications • Meningitis • Hydrocephalus • Encephalitis • Parenchymal cerebral or cerebellar abscesses • Occurrence in young children by haematogenous dissemination • Invasive organisms such as H. influenza type B more common • Neurologic sequalae of MR or SNHL
- 30. Carotid artery involvement • Exceptional in the AB era • Potential life threatening complication • Internal carotid more likely to be involved • Due to large no of lymph nodes adherent to ICA • Spread of infxn from adjacent IJV most likely to be mechanism of infection
- 31. • Protracted clinical course • Recurrent haemorrhage from Throat, nose or ear • Horner syndrome • Diagnosis often made at an advanced stage, when patient develops haemorrhage, pseudo aneurysm or hemiplegia • MR angiography most helpful and can show features of carotid artery spasm • Worst scenario – carotid occlusion /rupture
- 32. Other Head &Neck complications • Bezold abscess • along the medial aspect of mastoid tip up to sheath of SCN • Citelli’s abscess • along posterior belly of digastric • Luc’s abscess • along the posterior wall of the external auditory canal • Para pharyngeal and retropharyngeal abscess • Case in literature due to spread of the infection along the EU tube and spreading into the Retropharyngeal and Para pharyngeal spaces
- 33. Bezold Abscess • Occurs as a result of osteolysis at the mastoid tip • The pus/debris may extend inferiorly into the soft tissue of the neck and form an abscess • Aeration of mastoid bone with resulting thinning of osseous walls is believed to be predisposing factor for bezold abscess • Incomplete mastoid pneumatisation in infancy and early childhood is responsible for rare appearance in children • Very few cases reported in children under 5 years of age
- 34. Diagnosis??
Notas del editor
- Temporal bone: 5 parts Squamous portion biggest part and lies superior to all Posterior and inf to squamous portion mastoid portion Fused wit squamous and mastoid part and btwn sphenoid and occipital bone is petrous portion Recognisable because of it’s pyramid shape Tympanic part is small portion inferior to sq portion, anterior to mastoid, sup to styloid process Styloid, long pointed process, directed downwards, forwards and medially between parotid and IJV (thorn shaped)
- Mastoid part is pneumatised by mastoid air cells Outer rough surface which provides attachment to occipitalis and auricularis, Continues inferiorly as mastoid process, a conical bony projection for the above muscles Medial aspect of mastoid process is digastric groove, medial to this groove is occipital groove for occipital artery Sigmoid sulcus which lodges part of transverse sinus lies in the inner surface of the mastoid portion of temp bone
- More than half of the strept pneumonia recovered are serotype 19, 23 and 3 High frequency of MRDSP is now associated with AM and this may alter selection of AB 40 – 50% are Penicillin resistant, 25% ceftriaxone resistant Gm neg organisms and Staph Aureus recovered more frequently from pt with chronic mastoiditis
- Audio done during and after mastoiditis help to quantify and monter any associated hearing loss
- More common in acute infection. Lateral sinus thrombophlebitis causes spread of infection to the cerebellum
- The osteoclastic osseous reabsorption proceeds in all directions and have higher probability of intracranial complications before resolution
- Management of coalescent mastoiditis is controversial Options are AB’s alone, AB plus myringotomy – can resolve uncomplicated or incipient mastoiditis I & D of supberiosteal abscess Mastiodectomy – goal of surgery is effective drainage that eliminates the oedema and granulation in the aditus ad antrum and establish good communication btw middle ear and mastoid Clinical indications for surgery include absence of clinical recovery after 24/48 hrs of ivi meds Evidence of mastoid coalescence at temporal bone CT Or progression of symptoms in a patient in whom conservative management was initiated
- 30% of population have pnematized petrous apex Gradenigo’s syndrome pain in orbit or behind the eye (trigeminal ganclionitis, abducence palsy, often 2,3,7,8,9 and 10 may be involved. Extension of infection from middle ear and mastoid air cells into pneumatized petrous apex via the perilabyrithine air tracts Differential diagnosis neoplastic disease ( rhabdomyosarcoma or metastasis or epidermoid tumours)
- 7 year old girl with fever right sided facial pain, diplopia Axial ct show increased attenuation of the mastoid air cells wand erosion of right petrous apex, with well pneumatized left petroux apex, contrast ct shows hypo attenuated mass no soft tissue involvement. Mri C – low and high signal intensity Pt treated with mastoidectomy for drainage and ivi meds
- Facial nerve paralysis often affects the tympanic and upper mastoid segments Lesion is often not destructive and reversible (unless TB mastoiditis or malignancy)
- Epidural abscess with sigmoid sinus phlebothrombosis in 3 year old child with acute mastoiditis and no neurologic symptoms Axial ct shows increased attenuation of right middle ear with a large osseous defect over the sigmoid sinus plate, contrast ct shows epidural Since introduction of AB’s the incidence has reduced Due to the infection itself 2. Due to compression of the brain tissue high index of suspicion and early diagnosis essential because of high mortality Early symptoms_ increased otorrhoea, fever, headache altered mental status, CN palsy and signs of meningitis Trautmann triangle:
- Less common mechanism or Dural thrombosis may be osteothrombophlebitis with intact osseous plate Indirect imaging show signs of Dural venous thrombosis = low attenuation of sinus on unenhanced and contrast enhanced ct Absence of normal flow on spin echo MRI and absence of flow related enhancement
- 4 years female with left acute mastoiditis. Increased attenuation of left mastoid with a clear defect in the posterior and lateral mastoid cortex Contrast ct shows asymmetric enhancement of sigmoid sinus Axial MR venogram shows absence of normal venous flow with occlusion at the level of mid transverse sinus and some evidence of collaterals
- Patients usually meningism Focal neurological signs Seizures Often present to neurosurgeons 1st
- 3 yrs female with left acute mastoiditis with lethargy, stiff neck and headache Uncontrasted ct scans show bilateral middle ear ds with no evidence of bony erosion, contrasted ct scan show fluid collection extending along the left tentorium cerebelli and post interhemispheric fissure Direct coronal contrast enhanced ct show continuity of both fluid collections as well as sub periosteal inflammatory soft tissue on left
- Citelli’s abscess - tracking of abscess deep into the neck along the posterior belly of digastric muscle. Patient may have facial nerve palsy if stylomastoid region inflamed/ affected by infxn Luc’s abscess –abscess tracks along the posterior wall of external auditory canal, may extend upward below the temporalis muscle