
Recomendados
Más contenido relacionado
La actualidad más candente
La actualidad más candente (20)
Destacado
Destacado (14)
Similar a Endocrine disorder
Similar a Endocrine disorder (20)
Más de specialclass
Más de specialclass (20)
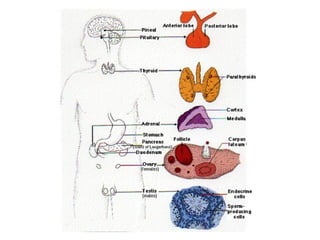
Endocrine disorder
- 2. Endocrine System Pituitary Gland - The main endocrine gland. - Called the “master” gland. - Acts as the control center for the endocrine system which controls all the hormones produced by other glands in the body.
- 5. Some of the neurons within the hypothalamus - neurosecretory neurons - secrete hormones that strictly control secretion of hormones from the anterior pituitary. The hypothalamic hormones are referred to as releasing hormones and inhibiting hormones, reflecting their influence on anterior pituitary hormones.
- 6. Hypothalamic releasing and inhibiting hormones are carried directly to the anterior pituitary gland via hypothalamic- hypophyseal portal veins . Specific hypothalamic hormones bind to receptors on specific anterior pituitary cells, modulating the release of the hormone they produce.
- 8. Anterior Pituitary Posterior pituitary Stimulates milk ejection and uterine contractions Ovary and testisOxytocin Conservation of body water KidneyAntidiuretic hormone Control of reproductive function Ovary and testisFollicle stimulating hormone Control of reproductive function Ovary and testisLuteinizing hormone Milk productionMammary glandProlactin Stimulates secretion of glucocorticoids Adrenal gland cortexAdrenocorticotrophic hormone Stimulates secretion of thyroid hormones Thyroid glandThyroid stimulating hormone Promotes growth (indirectly), control of protein, lipid and carbohydrate metabolism Liver, adipose tissueGrowth hormone Major physiologic effects Major target organsHormone
- 9. • The portion of the adenohypophysis known as the pars tuberalis contains cords of epithelial cells and is filled with hypophyseal portal vessels. It reportedly contains gonadotropes and thyrotropes, plus other secretory cells of unknown function. • The pars intermedia is closely associated with pars nervosa and separated from the pars distalis by the hypophyseal cleft. Melanocyte-stimulating hormone is the predominant hormone secreted by the pars intermedia. The pituitary gland has two distinct parts, the anterior and the posterior lobes, each of which releases different hormones.
- 10. • Histology of the Adenohypophysis • The bulk of the adenohypophysis is pars distalis. That tissue is composed of winding cords of epithelial cells flanked by vascular sinusoids. • In sections stained with dyes such as hematoxylin and eosin, three distinct cell types are seen among epithelial cells: • Acidophils have cytoplasm that stains red or orange • Basophils have cytoplasm that stains a bluish color • Chromophobes have cytoplasm that stains very poorly
- 11. • Histology of the Adenohypophysis • The bulk of the adenohypophysis is pars distalis. That tissue is composed of winding cords of epithelial cells flanked by vascular sinusoids. • In sections stained with dyes such as hematoxylin and eosin, three distinct cell types are seen among epithelial cells: • Acidophils have cytoplasm that stains red or orange • Basophils have cytoplasm that stains a bluish color • Chromophobes have cytoplasm that stains very poorly
- 12. Acidophils: contain the polypeptide hormones: – Somatotropes which produce growth hormone – Lactotropes which produce prolactin Basophils: contain the glycoprotein hormones: – Thyrotropes which produce thyroid stimulating hormone – Gonadotropes which produce luteinizing hormone or follicle-stimulating hormone – Corticotropes which produce adrenocorticotrophic hormone Chromophobes • These are cells that have minimal or no hormonal content. – may be acidophils or basophils that have degranulated and thereby are depleted of hormone – may also represent stem cells that have not yet differentiated into hormone-producing cells.
- 13. • Although classification of cells as acidophils or basophils is useful in some situations, specific identification of anterior pituitary cells requires immunostaining for the hormone in question. • In addition to differential staining characteristics, the size of secretory granules varies among different types of cells in the anterior pituitary. Somatotropes and lactotropes tend to have the largest size granules.
- 15. Pituitary tumor causes symptoms by any of three mechanisms: 1. By producing too much of one or more hormones. 2. By compressing the pituitary gland, and thus making it produce too little of one or more hormones. 3. By compressing the optic nerves or (less commonly) the nerves controlling eye movements, and thus causing either loss of part or all of the visual field, or double vision.
- 19. Type of Adenoma Secretion Staining Pathology Corticotrophic adenomas Secrete adrenocotrophic hormone (ACTH) and Proopiomelanocortin (POCM) Basophilic Cushing’s disease Somatotrophic adenomas Secrete growth hormone (GH) Acidophilic Acromegaly (Gigantism) Thyrotrophic adenomas (rare) Secret thyroid stimulating hormone (TSH) Basophilic Occasionally hyperthyroidism usually does not cause symptoms Gonadotrophic adenomas Secrete luteinizing hormone (LH), follicle stimulating hormone (FSH) Basophilic Usually does not cause symptoms Prolactinomas Secret prolactin Acidophilic Galactorrhea, hypogonadism, amenorrhea, infertility and impotence Null cells adenomas Do not secrete hormones May stain positive for synaptophysin
- 20. By producing too much of one or more hormones • Growth hormone: causes ACROMEGALY – a syndrome that includes: • excessive growth of soft tissues and bones • high blood sugar • high blood pressure • heart disease • sleep apnea • excess snoring • carpal tunnel syndrome • pain symptoms (including headache).
- 21. By producing too much of one or more hormones • Thyroid stimulating hormone: – causes high production of thyroid hormone – Thyroid hormone: • leads to nervousness and irritability • fast heart rate and high blood pressure • heart disease • excess sweating and thin skin • and weight loss.
- 22. By producing too much of one or more hormones • Prolactin: – causes inappropriate secretion of breast milk (even in men) – osteoporosis (bone weakening) – loss of sex drive – Infertility – irregular menstrual cycles – and impotence
- 23. By producing too much of one or more hormones • Adrenocorticotropic hormone: – causes weight gain (particularly in the body’s trunk, not the legs or arms) – high blood pressure – high blood sugar – brittle bones – emotional changes – stretch marks on the skin – easy bruising.
- 24. By producing too much of one or more hormones • Gonadotropins (FSH and LH): – usually not elevated enough to produce direct symptoms – but in extreme cases can cause infertility (inability to have a child) – irregular menstrual cycles in women.
- 25. Cushing’s Syndrome • Definition – a condition that occurs when your body is exposed to high levels of the hormone cortisol for a long time. – Referred to as hypercortisolism – use of oral corticosteroid medication (most common cause) – The condition can also occur when your body makes too much cortisol.
- 26. Hallmark signs of Cushing's syndrome: - fatty hump between shoulders - rounded face - pink or purple stretch marks on your skin - can also result in high blood pressure, bone loss and, on occasion, diabetes.
- 27. By compressing the pituitary gland, and thus making it produce too little of one or more hormones. • Growth hormone: causes poor muscle strength, irritability, weakening of bone strength, and overall feeling of malaise (feeling unwell). DWARFISM in children. Thyroid stimulating hormone: causes fatigue, low energy, and weight gain. • Prolactin: causes inability to breastfeed after a woman gives birth to a baby. • Adrenocorticotropic hormone: causes fatigue and low energy, low blood pressure, low blood sugar, and upset stomach. • Gonadotropins (FSH and LH): cause infertility, decrease in sex drive, impotence, and irregular menstrual cycles.
- 28. Histology of the Neurohypophysis • The neurohypophysis is known also as the pars nervosa. • Three areas of this organ, starting closest to the hypothalamus: – the median eminence – infundibular stalk – infundibular process • The infundibular - bulk of the neurohypophysis (usually referred to as the posterior pituitary) • Composed on largely unmyelinated axons from hypothalamic neurosecretory neurons. • These neurons secrete oxytocin and antidiuretic hormone.
- 29. • The neurohypophysis shown here resembles neural tissue, with glial cells, nerve fibers, nerve endings, and intra-axonal neurosecretory granules. • The hormones vasopressin (antidiuretic hormone, or ADH) and oxytocin made in the hypothalamus (supraoptic and paraventricular nuclei) are transported into the intra-axonal neurosecretory granules where they are released.
- 30. Anterior pituitary Posterior pituitary
- 31. • Oxytocin increases uterine contractions and stimulates milk secretion. • Underproduction of ADH results in a disorder called diabetes insipidus characterized by inability to concentrate the urine. The consequence is excess urination leading potentially to dehydration. • Antidiuretic hormone (ADH) increases reabsorption of water by the tubules of the kidney.
- 32. Syndrome of Inappropriate ADH Secretion (SIADH) = Excess resorption of water -> hyponatremia = CAUSES: Secretion of ectopic ADH (small cell ca of the lung) Injury to hypothalamus or pituitary or both.
- 33. Parathyroid Gland They are hard to differentiate from the thyroid or fat. The parathyroid glands are four or more small glands, about the size of a grain of rice, located on the posterior surface (back side) of the thyroid gland. The parathyroid glands are named for their proximity to the thyroid but serve a completely different role than the thyroid gland. They are quite easily recognizable from the thyroid as they have densely packed cells, in contrast with the follicle structure of the thyroid.
- 34. Thyroid Gland: colloid-filled follicles Parathyroid Gland
- 35. The sole purpose of the parathyroid glands is to control calcium within the blood in a very tight range between 8.5 and 10.5. Parathyroid hormone (PTH) - mobilizes calcium release from bone when there is a decrease the blood level of calcium. - enhances intestinal absorption of calcium. PARATHYROID HORMONE
- 36. Hyperparthyroidism • The most common cause of excess hormone production (hyperparathyroidism) is the development of a benign tumor in one of the parathyroid glands. • Over-production of parathyroid hormone. • Occur in 94 percent of all patients with primary hyperparathyroidism.
- 38. Hyperprathyroidism Symptoms of Parathyroid Disease • Loss of energy. • Don't feel like doing much. Tired all the time. • Just don't feel well; don't quite feel normal. Hard to explain but just feel kind of bad. • Feel old. Don't have the interest in things that you used to. • Can't concentrate, or can't keep your concentration like in the past. • Depression. • Osteoporosis and Osteopenia. Bones hurt; typically it's bones in the legs and arms but can be most bones. • Don't sleep like you used to. Wake up in middle of night. Trouble getting to sleep. • Tired during the day and frequently feel like you want a nap. • Spouse claims you are more irritable and harder to get along with (cranky, bitchy). • Forget simple things that you used to remember very easily. • Gastric acid reflux; heartburn; GERD. • Decrease in sex drive. • Thinning hair (predominately in older females). • Kidney Stones. • High Blood Pressure (sometimes mild, sometimes quite severe; up and down a lot). • Recurrent Headaches (usually patients under the age of 40). • Heart Palpitations (arrhythmias). Typically atrial arrhythmias.
- 40. Adrenal Glands
- 41. • Located immediately anterior to the kidneys, encased in a connective tissue capsule and usually partially buried in an island of fat. • Retroperitoneal.
- 43. Adrenal Gland Adrenal cortex - secretes several classes of steroid hormones (glucocorticoids and mineralocorticoids) - with three concentric zones of cells that differ in the major steroid hormones they secrete.
- 44. Adrenal Gland Adrenal medulla - source of the catecholamines epinephrine and norepinephrine. - chromaffin cell is the principle cell type. - The medulla is richly innervated by preganglionic sympathetic fibers and is, in essence, an extension of the sympathetic nervous system.
- 45. HORMONE SYNTHESIS: – Corticosteroid. – Androgen such as testoterone. – Aldosterone. – Function is regulated by the neuroendocrine hormones from the pituitary, hypothalamus and renin-angiotensin system. – Adrenal medulla is regulated by direct innervation. ADRENAL CORTEX
- 46. The adrenal cortex comprises three zones each produces and secretes distinct hormones. • Zona glomerulosa (outer) – for production of mineralocorticoids, mainly aldosterone, which is largely responsible for the long-term regulation of blood pressure. • Zona fasciculata – responsible for producing glucocorticoids, chiefly cortisol in humans. • Zona reticularis (innermost) – produces androgens, mainly dehydroepiandrosterone (DHEA) and DHEA sulfate (DHEA-S) in humans. ADRENAL CORTEX
- 47. Adrenal Medullary Hormones – Cells in the adrenal medulla synthesize and secrete epinephrine and norepinephrine. Adrenergic Receptors and Mechanism of Action – The physiologic effects of epinephrine and norepinephrine are initiated by their binding to adrenergic receptors on the surface of target cells.
- 48. Receptor Effectively Binds Effect of Ligand Binding Alpha1 Epinephrine, Norepinephrine Increased free calcium Alpha2 Epinephrine, Norepinephrine Decreased cyclic AMP Beta1 Epinephrine, Norepinephrine Increased cyclic AMP Beta2 Epinephrine Increased cyclic AMP
- 49. Adrenal cortical hyperplasia. causes: - due to a pituitary adenoma secreting ACTH (Cushing's disease) - Cushing's syndrome from ectopic ACTH production - idiopathic adrenal hyperplasia. Adrenal atrophy (with either Addison's disease or long- term corticosteroid therapy). Normal adrenal glands
- 50. Adrenal adenoma with Cushing's syndrome - remaining atrophic adrenal is seen at the right. - composed of yellow firm tissue just like adrenal cortex. - well-circumscribed. Histologically - composed of well-differentiated cells resembling cortical fasciculata zone. It is benign.
- 51. Hallmark signs of Cushing's syndrome: - fatty hump between shoulders - rounded face - pink or purple stretch marks on your skin - can also result in high blood pressure, bone loss and, on occasion, diabetes.
- 52. PRIMARY HYPERALDOSTERONISM • Generic term for a closely related, uncommon syndromes characterized by chronic excess aldosterone secretion independent of the RA system. • Characterized by suppression of plasma renin activity. • Secondary increased aldostrerone due to renal ischemia (2ndary hyperladosteronism)
- 53. Causes of Primary Hyperaldosteronism 1. Conn’s Syndrome: -solitary aldosterone-secreting adenoma 2. Bilateral Idiopathic Hyperplasia of adrenals. 3. Glucocorticoid-suppressible hyperaldosteronism 4. Adrenal Cortical Carcinoma
- 54. Solitary aldosterone secreting adenoma - Conn’s Syndrome - patient had hypokalemia. - with high serum aldosterone and a low serum renin, - This lesion accounts for about two-thirds of cases of primary hyperaldosteronism (PHA) - Bilateral adrenal hyperplasia accounts for about 30% of PHA.
- 55. • Microscopically, the adrenal cortical adenoma at the right resembles normal adrenal fasciculata. The capsule is at the left. There may be some cellular pleomorphism.
- 56. • This is a large adrenal cortical carcinoma which is displacing the left kidney downward. • Such neoplasms are usually functional (secreting corticosteroids or sex steroids). • They have a poor prognosis.
- 57. • High power microscopic appearance of an adrenal cortical carcinoma • loosely resembles normal adrenal cortex • It is difficult to determine malignancy in endocrine neoplasms based upon cytology alone. • Thus, invasion (as seen here in a vein) and metastases are the most reliable indicators. • Luckily, most endocrine neoplasms are benign adenomas. BV TC
- 58. • Here is an adrenal cortical carcinoma seen microscopically at high power to demonstrate cellular pleomorphism with nuclear hyperchromatism. • Both benign and malignant endocrine neoplasms demonstrate some degree of cellular pleomorphism, so it is not easy to tell benign from malignant on histologic grounds alone. The larger the neoplasm, the more likely it is malignant, but the best indicators are invasion and metastasis.
- 59. ADRENAL MEDULLA A. PHEOCHROMOCYTOMA: - associated with catecholamine-induced hypertension. - occassionally, this tumor produces other biogenic steroids or peptides asociated with Cushing’s Syndrome. -morphology: - ave . weight of 100 gms - Zellballen appearance
- 60. • This large adrenal neoplasm has been sectioned in half. Note the grey-tan color of the tumor compared to the yellow cortex stretched around it and a small remnant of remaining adrenal at the lower right. This patient had episodic hypertension. This is a tumor arising in the adrenal medulla--a pheochromocytoma. T N
- 61. • There is some residual adrenal cortical tissue at the lower center right, with the darker cells of pheochromocytoma seen above and to the left.
- 62. HYPOADRENALISM • Caused by any anatomic or metabolic lesion of the adrenal cortex that impairs output of the cortical steroids. • Primary Acute Adrenal Insufficiency - Waterhouse Friderichsen Syndrome due to overwhelming septicemic infection caused by meningococci but occasionally other virulent organism such as gonococci,pneumococi and staphylococci. morphology: massive bilateral adrenal hemorrhage
- 63. HYPOADRENALISM • Primary Chronic Adrenal Insufficiency: - Addison’s Disease - caused by any destructive process in the adrenal cortex. a. Autoimmune Adrenalitis b. Infection c. Metastatic Ca to the adrenal cortex