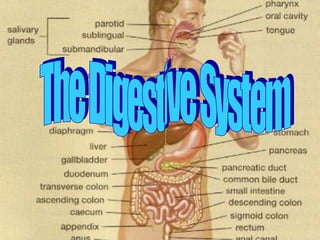
Digestion involves the mixing of food, its movement through the digestive tract, and the chemical breakdown of the large molecules of food into smaller molecules. Digestion begins in the mouth, when we chew and swallow, and is completed in the small intestine. The chemical process varies somewhat for different kinds of food. Movement of Food Through the System The large, hollow organs of the digestive system contain muscle that enables their walls to move. The movement of organ walls can propel food and liquid and also can mix the contents within each organ. Typical movement of the esophagus, stomach, and intestine is called peristalsis. The action of peristalsis looks like an ocean wave moving through the muscle. The muscle of the organ produces a narrowing and then propels the narrowed portion slowly down the length of the organ. These waves of narrowing push the food and fluid in front of them through each hollow organ. The first major muscle movement occurs when food or liquid is swallowed. Although we are able to start swallowing by choice, once the swallow begins, it becomes involuntary and proceeds under the control of the nerves. The esophagus is the organ into which the swallowed food is pushed. It connects the throat above with the stomach below. At the junction of the esophagus and stomach, there is a ringlike valve closing the passage between the two organs. However, as the food approaches the closed ring, the surrounding muscles relax and allow the food to pass. The food then enters the stomach, which has three mechanical tasks to do. First, the stomach must store the swallowed food and liquid. This requires the muscle of the upper part of the stomach to relax and accept large volumes of swallowed material. The second job is to mix up the food, liquid, and digestive juice produced by the stomach. The lower part of the stomach mixes these materials by its muscle action. The third task of the stomach is to empty its contents slowly into the small intestine. Several factors affect emptying of the stomach, including the nature of the food (mainly its fat and protein content) and the degree of muscle action of the emptying stomach and the next organ to receive the contents (the small intestine). As the food is digested in the small intestine and dissolved into the juices from the pancreas, liver, and intestine, the contents of the intestine are mixed and pushed forward to allow further digestion. Finally, all of the digested nutrients are absorbed through the intestinal walls. The waste products of this process include undigested parts of the food, known as fiber, and older cells that have been shed from the mucosa. These materials are propelled into the colon, where they remain, usually for a day or two, until the feces are expelled by a bowel movement. Production of Digestive Juices The glands that act first are in the mouth—the salivary glands. Saliva produced by these glands contains an enzyme that begins to digest the starch from food into smaller molecules. The next set of digestive glands is in the stomach lining. They produce stomach acid and an enzyme that digests protein. One of the unsolved puzzles of the digestive system is why the acid juice of the stomach does not dissolve the tissue of the stomach itself. In most people, the stomach mucosa is able to resist the juice, although food and other tissues of the body cannot. After the stomach empties the food and juice mixture into the small intestine, the juices of two other digestive organs mix with the food to continue the process of digestion. One of these organs is the pancreas. It produces a juice that contains a wide array of enzymes to break down the carbohydrate, fat, and protein in food. Other enzymes that are active in the process come from glands in the wall of the intestine or even a part of that wall. The liver produces yet another digestive juice—bile. The bile is stored between meals in the gallbladder. At mealtime, it is squeezed out of the gallbladder into the bile ducts to reach the intestine and mix with the fat in our food. The bile acids dissolve the fat into the watery contents of the intestine, much like detergents that dissolve grease from a frying pan. After the fat is dissolved, it is digested by enzymes from the pancreas and the lining of the intestine. Absorption and Transport of Nutrients Digested molecules of food, as well as water and minerals from the diet, are absorbed from the cavity of the upper small intestine. Most absorbed materials cross the mucosa into the blood and are carried off in the bloodstream to other parts of the body for storage or further chemical change. As already noted, this part of the process varies with different types of nutrients. Carbohydrates. It is recommended that about 55 to 60 percent of total daily calories be from carbohydrates. Some of our most common foods contain mostly carbohydrates. Examples are bread, potatoes, legumes, rice, spaghetti, fruits, and vegetables. Many of these foods contain both starch and fiber. The digestible carbohydrates are broken into simpler molecules by enzymes in the saliva, in juice produced by the pancreas, and in the lining of the small intestine. Starch is digested in two steps: First, an enzyme in the saliva and pancreatic juice breaks the starch into molecules called maltose; then an enzyme in the lining of the small intestine (maltase) splits the maltose into glucose molecules that can be absorbed into the blood. Glucose is carried through the bloodstream to the liver, where it is stored or used to provide energy for the work of the body. Table sugar is another carbohydrate that must be digested to be useful. An enzyme in the lining of the small intestine digests table sugar into glucose and fructose, each of which can be absorbed from the intestinal cavity into the blood. Milk contains yet another type of sugar, lactose, which is changed into absorbable molecules by an enzyme called lactase, also found in the intestinal lining. Protein. Foods such as meat, eggs, and beans consist of giant molecules of protein that must be digested by enzymes before they can be used to build and repair body tissues. An enzyme in the juice of the stomach starts the digestion of swallowed protein. Further digestion of the protein is completed in the small intestine. Here, several enzymes from the pancreatic juice and the lining of the intestine carry out the breakdown of huge protein molecules into small molecules called amino acids. These small molecules can be absorbed from the hollow of the small intestine into the blood and then be carried to all parts of the body to build the walls and other parts of cells. Fats. Fat molecules are a rich source of energy for the body. The first step in digestion of a fat such as butter is to dissolve it into the watery content of the intestinal cavity. The bile acids produced by the liver act as natural detergents to dissolve fat in water and allow the enzymes to break the large fat molecules into smaller molecules, some of which are fatty acids and cholesterol. The bile acids combine with the fatty acids and cholesterol and help these molecules to move into the cells of the mucosa. In these cells the small molecules are formed back into large molecules, most of which pass into vessels (called lymphatics) near the intestine. These small vessels carry the reformed fat to the veins of the chest, and the blood carries the fat to storage depots in different parts of the body. Vitamins. Another vital part of our food that is absorbed from the small intestine is the class of chemicals we call vitamins. The two different types of vitamins are classified by the fluid in which they can be dissolved: water-soluble vitamins (all the B vitamins and vitamin C) and fat-soluble vitamins (vitamins A, D, and K). Water and salt. Most of the material absorbed from the cavity of the small intestine is water in which salt is dissolved. The salt and water come from the food and liquid we swallow and the juices secreted by the many digestive glands.
The abdomen can be divided into quadrants or nine abdominal regions. Pain felt in these regions may be considered to be direct or referred. The midline in the sagittal plane is the linea alba . The lateral edge of the rectus sheath is the linea semilunaris. The lower costal margin, the iliac crest and public tubercle can be palpated. The abdominal wall is divided into four quadrants by a vertical and a horizontal line bisecting the umbilicus. An older more complicated scheme divided the abdomen into nine regions. Although the old system generally is not used, some regional names persist, such as epigastric for the area between the costal margins, umbilical for the area around the umbilicus, and hypogastric or suprapubic for the area above the pubic bone.
Preparation for Gastroscopy (EGD) An Important Exam Requires Careful Preparation The doctor has decided that gastroscopy is necessary to better evaluate your upper digestive tract. An important examination such as this requires proper preparation. The results obtained from this exam are dependent on your stomach being empty. Food particles inside the stomach can hide important conditions that may be present and may increase the risk of aspiration (choking) during the examination. Day Before Your Examination There are no restrictions on food, drink, or activity on the day before your test. Unlike colonoscopy, there is no laxative prep for this exam. Morning of the Examination Your stomach must be empty during gastroscopy so that your doctor's view is not blocked by particles of food. If your test is scheduled in the morning, you must not eat or drink anything after midnight the night before the test. You may gargle and brush your teeth in the morning. If your test is scheduled in the afternoon, you may have only liquids - such as juice, coffee, tea, or broth - for breakfast. Then begin fasting. You should not eat or drink anything for at least 6 hours before the exam. You may take all of your regular medications unless otherwise directed. No Insulin. If your are on Coumadin, ask for instructions several days before your appointment. You should arrive at the clinic at least 15 minutes before your scheduled appointment. We will complete your registration, have you change clothing, perform any pre-operative orders which might be required by your physician, and answer any questions you might have. Please be on time so that you don't cause a delay which could affect many other patients within the same day. Since sedation is utilized, YOU MUST BRING A COMPANION WITH YOU who is responsible and is able to drive you home after your procedure and to assist you with follow-up care. Only one companion is necessary, and we ask that they remain at the clinicr during your procedure and recovery which totals about 90 minutes. You will not be able to drive a car, operate any machinery, go to work or eat out at a restaurant until the following day.
From gihealth.com Strictures of the esophagus During a gastroscopy, we found spaghetti stuck in the esophagus
After removing the spaghetti, a meatball was found stuck below.
After we removed the meatball, we found this narrowed stricture.
Balloon dilator is inflated which stretches the narrow spot
Balloon dilator deflated and being withdrawn after dilating stricture
Flex sig movie from CD An Important Exam Requires Careful Preparation Your doctor has decided that flexible sigmoidoscopy is necessary to help him better evaluate your colon, or large intestine. An important exam such as this requires careful preparation. Accurate results from this exam require that your lower bowel (colon) is carefully cleansed and empty. An improperly prepared bowel may mean that the exam will have to be repeated at another time. More importantly, fecal matter (stool) left in the tract can hide important conditions that may be present. Therefore, it is very important that you follow these instructions as carefully as possible. No laxative preparation is fun. But this Ñprepæ has been developed to make your preparation as simple and effective as possible. Please follow each instruction exactly as given. Note that individual responses to laxatives vary widely. Remain within easy reach of toilet facilities. If you have any questions, please call the office. Several Days Before the Examination: Go to the drug store and purchase Two (2) Fleet Disposable Enemas (4 1/2 ounce) which will cost only a few dollars. You will NOT need a prescription. One Day Before the Examination: Eat normally. You may take all of your normal prescription medications. Please avoid Metamucil and foods with small seeds such as sesame seeds, kiwi, cucumbers for a few days before your exam. Day of the Examination About four hours before your exam, begin a clear liquid diet. The liquids you drink may be clear strained citrus juices, and other juices such as apple, cranberry, or grape, or simply plain water. Black coffee, tea, Jello (avoid red) or soft drinks are permissible. All solid foods, milk products, and alcohol should be avoided. About two hours before your exam use the first Fleet Disposable Enema. Shake bottle before using. Remove protective shield from rectal tip. Lie on your left side. Insert enema tip pointing toward navel. Squeeze bottle until nearly all liquid is expelled into rectum. Wait 15 minutes before evacuating, even if the urge is strong. About one hour before your exam use the second Fleet Disposable Enema. Shake bottle before using. Remove protective shield from rectal tip. Lie on your left side. Insert enema tip pointing toward navel. Squeeze bottle until nearly all liquid is expelled into rectum. Wait 15 minutes before evacuating, even if the urge is strong. If you have followed all instructions carefully, your system should be clean, clear and ready for examination. Report for your exam appointment as scheduled. Wear comfortable easily-folded clothing and leave jewelry and other valuables at home. If you have any questions please call our nurse at 412 262-1000 - select option #2 You should arrive at the Center at least 15 minutes before your scheduled appointment. We will complete your registration, have you change clothing, perform any pre-operative orders which might be required by your physician, and answer any questions you might have. Since sedation is not necessary for this simple exam, you will are not required to bring a driver. Please be on time so that you don't cause a delay which could affect many other patients within the same day.
Here is an example of what happens when someone abuses laxatives. The normal colon lining is pink and healthy looking. This 73 year old woman has taken laxatives almost every day for many years. At the time of colonoscopy, her colon showed a blackened appearance termed – Melanosis coli. These changes tell the doctor that the patient has abused laxatives for many years. Many people don’t realize that even non-prescription medications can lead to side effects if taken improperly. Some laxatives are dangerous to take on a regular basis. Some, like Metamucil or Citricel can be taken safely for years without danger. If you take non-fiber laxatives more often than once a week, you should discuss this with your physician.
Abdominal pain -- a dull ache, a burning sensation, or a sharp, stabbing pain -- is one of the most common complaints in all of medicine. Most people can blame abdominal pain on their stomachs, but the stomach is just one potential trouble spot. Any organ in your midsection can cause pain, including your appendix, gallbladder, pancreas, kidneys, and intestines. Heartburn Lying down after a big meal, you feel a burning pain in the center of your chest. Before long, the fire spreads upward to your neck. That searing pain you felt was heartburn, also known as acid indigestion Think of your stomach as a finely crafted container built to hold acid. As long as the container does its job, the acid isn't likely to cause any trouble. But the valve that connects the stomach to the esophagus sometimes leaks, allowing acid to splash upwards. Normally, everything that's in the stomach is kept from escaping upward by a band of muscle called the lower esophageal sphincter, or LES, located where the bottom of the esophagus intersects with the stomach. The LES valve opens when you're swallowing food, but otherwise is supposed to be clamped tight. If it begins to open too easily, the contents of the stomach -- food or acid -- can back up into the esophagus. The esophagus isn't designed to handle acid, so the leakage usually causes discomfort and a burning pain. Most people have heartburn every once in awhile. But if acid frequently escapes into the esophagus, the pain will be a regular part of your patient’s life. Nausea is the sensation of being about to vomit. Vomiting, or emesis, is the expelling of undigested food through the mouth. Nausea is a reaction to a number of causes that include overeating, infection, or irritation of the throat or stomach lining. Persistent or recurrent nausea and vomiting should be checked by a doctor. Persistent, unexplained, or recurring nausea and vomiting can be symptoms of a variety of serious illnesses. It can be caused by simply over-eating or drinking too much alcohol. It can be due to stress, medication, or illness. Morning sickness is a consequence of pregnancy-related hormone changes. Motion sickness can be induced by traveling in a vehicle, plane, or on a boat. Many patients experience nausea after eating spoiled food or foods to which they are allergic. Patients who suffer migraine headache often experience nausea. Cancer patients on chemotherapy are nauseated. Gallstones, gastroenteritis and stomach ulcer may cause nausea and vomiting. Flatulence Gas forms from a number of sources -- most commonly from swallowed air or as a byproduct from foods that are broken down and mixed with normal bacteria in the colon or large intestine. Gas from swallowed air -- made up of oxygen, nitrogen, and carbon dioxide -- usually ends up in the stomach. Most swallowed air is released through burping, though some of it travels downward through the intestines and is released through the rectum. If you think you have excessive gas, consider that most people pass gas at least 14 times a day Chronic, excessive gas could be a symptom of a serious disorder. In most cases, however, excess gas and any discomfort caused by it is highly treatable, often simply by paying more attention to what you eat, reducing the amount of air you swallow, and making some other lifestyle changes. Diarrhea occurs because more fluid passes through the large intestine (colon) than that organ can absorb. As a rule, the colon can absorb several times more fluid than is required on a daily basis. However, when this reserve capacity is overwhelmed, diarrhea occurs. Diarrhea is caused by infections or illnesses that either lead to excess production of fluids or prevent absorption of fluids. Also, certain substances in the colon, such as fats and bile acids, can interfere with water absorption and cause diarrhea. In addition, rapid passage of material through the colon can also do the same Constipation is one of the most common medical complaints in the United States. Constipation can occur at any age, and is more common among individuals who resist the urge to move their bowels at their body's signal. This often happens when children start school or enter daycare and feel shy about asking permission to use the bathroom. Constipation is more common in women than in men and is especially apt to occur during pregnancy. Age alone does not increase the frequency of constipation, but elderly people (especially women) are more likely to suffer from constipation. Hiccup is an involuntary spasmodic contraction of the diaphragm in which the beginning of an inspiration is suddenly checked by closure of the glottis. Hiccups can be caused by central nervous system disorders, injury or irritation to the phrenic and vagus nerves, and toxic or metabolic disorders affecting the central or peripheral nervous systems. They may be of unknown cause or may be a symptom of psychological stress. Hiccups often occur after drinking carbonated beverages or alcohol. They may also follow overeating or rapid temperature changes.
Cirrhosis changes the structure of the liver and the blood vessels that nourish it. The disease reduces the liver's ability to manufacture proteins and process hormones, nutrients, medications, and poisons. Cirrhosis gets worse over time and can become potentially life threatening. This disease can cause: excessive bleeding (hemorrhage) impotence liver cancer coma due to accumulated ammonia and body wastes (liver failure) sepsis (blood poisoning) Death. Cirrhosis is the seventh leading cause of disease-related death in the United States. It is the third most common cause of death in adults between the ages of 45 and 65. It is twice as common in men as in women. The disease occurs in more than half of all malnourished chronic alcoholics, and kills about 25,000 people a year. In Asia and Africa, however, most deaths from cirrhosis are due to chronic hepatitis B. Portal or nutritional cirrhosis is the form of the disease most common in the United States. About 30-50% of all cases of cirrhosis are this type. Nine out of every 10 people who have nutritional cirrhosis have a history of alcoholism. Biliary cirrhosis is caused by intrahepatic bile-duct diseases that impede bile flow. Bile is formed in the liver and is carried by ducts to the intestines. Bile then helps digest fats in the intestines. Biliary cirrhosis can scar or block these ducts. It represents 15-20% of all cirrhosis. Various types of chronic hepatitis, especially hepatitis B and hepatitis C, can cause postnecrotic cirrhosis. This form of the disease affects up to 40% of all patients who have cirrhosis. As the disease progresses, the spleen enlarges and fluid collects in the abdomen (ascites) and legs (edema). Spider-like blood vessels appear on the chest and shoulders, and bruising becomes common. Men sometimes lose chest hair. Their breasts may grow and their testicles may shrink. Women may have menstrual irregularities. Cirrhosis can cause extremely dry skin and intense itching. The whites of the eyes and the skin may turn yellow (jaundice), and urine may be dark yellow or brown. Stools may be black or bloody. Sometimes the patient develops persistent high blood pressure due to the scarring (portal hypertension). This type of hypertension can be life threatening. It can cause veins to enlarge in the stomach and in the tube leading from the mouth to the stomach (esophagus). These enlarged veins are called varices, and they can rupture and bleed massively. Alcohol Metabolism. Most of the alcohol a person drinks is eventually broken down by the liver. However, some products generated during alcohol metabolism (e.g., acetaldehyde) are more toxic than alcohol itself. In addition, a group of metabolic products called free radicals can damage liver cells and promote inflammation, impairing vital functions such as energy production. The body's natural defenses against free radicals (e.g., antioxidants) can be inhibited by alcohol consumption, leading to increased liver damage (3). The Inflammatory Response. Inflammation is the body's response to local tissue damage or infection. Inflammation prevents the spread of injury and mobilizes the defense mechanisms of the immune system. One such defense mechanism is the generation of free radicals that can destroy disease-causing microorganisms. Long-term alcohol consumption prolongs the inflammatory process, leading to excessive production of free radicals, which can destroy healthy liver tissue. Bacteria that live in the human intestine play a key role in the initiation of ALD. Alcohol consumption increases the passage of a noxious bacterial product called endotoxin through the intestinal wall into the bloodstream. Upon reaching the liver, endotoxin activates specialized cells (i.e., Kupffer cells) that monitor the blood for signs of infection. These cells respond to the presence of endotoxin by releasing substances called cytokines that regulate the inflammatory process (4-6). Cytokines. Cytokines are produced by cells of the liver and immune system in response to infection or cell damage. Alcohol consumption increases cytokine levels, and cytokines in humans produce symptoms similar to those of alcoholic hepatitis (7). Recent studies implicate cytokines in scar formation and in the depletion of oxygen within liver cells, processes that are associated with cirrhosis (7). Each of the disease mechanisms described above contributes to the death of liver cells. The presence of damaged cells triggers the body's defensive responses, including the release of additional cytokines, resulting in a vicious cycle of inflammation, cell death, and scarring. Scar Formation. Normal scar formation is part of the wound-healing process. Alcohol-induced cell death and inflammation can result in scarring that distorts the liver's internal structure and impairs its function. This scarring is the hallmark of cirrhosis. The process by which cirrhosis develops involves the interaction of certain cytokines and specialized liver cells (i.e., stellate cells). In the normal liver, stellate cells function as storage depots for vitamin A. Upon activation by cytokines, stellate cells proliferate, lose their vitamin A stores, and begin to produce scar tissue. In addition, activated stellate cells constrict blood vessels, impeding the delivery of oxygen to liver cells (6,8). Acetaldehyde may activate stellate cells directly, promoting liver scarring in the absence of inflammation (9,10). This finding is consistent with the observation that heavy drinkers can develop cirrhosis insidiously, without preexisting hepatitis.
Play Dormia Basket CD A gallstone is a solid crystal deposit that forms in the gallbladder, which is a pear-shaped organ that stores bile salts until they are needed to help digest fatty foods. Gallstones can migrate to other parts of the digestive tract and cause severe pain with life-threatening complications. Gallstones vary in size and chemical structure. A gallstone may be as tiny as a grain of sand or as large as a golf ball. Eighty percent of gallstones are composed of cholesterol. They are formed when the liver produces more cholesterol than digestive juices can liquefy. The remaining 20% of gallstones are composed of calcium and an orange-yellow waste product called bilirubin. Bilirubin gives urine its characteristic color and sometimes causes jaundice. Gallstones are the most common of all gallbladder problems. They are responsible for 90% of gallbladder and bile duct disease, and are the fifth most common reason for hospitalization of adults in the United States. Gallstones usually develop in adults between the ages of 20 and 50; about 20% of patients with gallstones are over 40. The risk of developing gallstones increases with age--at least 20% of people over 60 have a single large stone or as many as several thousand smaller ones. The gender ratio of gallstone patients changes with age. Young women are between two and six times more likely to develop gallstones than men in the same age group. In patients over 50, the condition affects men and women with equal frequency. Native Americans develop gallstones more often than any other segment of the population; Mexican-Americans have the second-highest incidence of this disease. Gallstones can cause several different disorders. Cholelithiasis is defined as the presence of gallstones within the gallbladder itself. Choledocholithiasis is the presence of gallstones within the common bile duct that leads into the first portion of the small intestine (the duodenum). The stones in the duct may have been formed inside it or carried there from the gallbladder. These gallstones prevent bile from flowing into the duodenum. Ten percent of patients with gallstones have choledocholithiasis, which is sometimes called common-duct stones. Patients who don't develop infection usually recover completely from this disorder. Cholecystitis is a disorder marked by inflammation of the gallbladder. It is usually caused by the passage of a stone from the gallbladder into the cystic duct, which is a tube that connects the gallbladder to the common bile duct. In 5-10% of cases, however, cholecystitis develops in the absence of gallstones. This form of the disorder is called acalculous cholecystitis. Cholecystitis causes painful enlargement of the gallbladder and is responsible for 10-25% of all gallbladder surgery. Chronic cholecystitis is most common in the elderly. The acute form is most likely to occur in middle-aged adults. Cholesterolosis or cholesterol polyps is characterized by deposits of cholesterol crystals in the lining of the gallbladder. This condition may be caused by high levels of cholesterol or inadequate quantities of bile salts, and is usually treated by surgery. Gallstone ileus, which results from a gallstone's blocking the entrance to the large intestine, is most common in elderly people. Surgery usually cures this condition. Narrowing (stricture) of the common bile duct develops in as many as 5% of patients whose gallbladders have been surgically removed. This condition is characterized by inability to digest fatty foods and by abdominal pain, which sometimes occurs in spasms. Patients with stricture of the common bile duct are likely to recover after appropriate surgical treatment. Gallstones are caused by an alteration in the chemical composition of bile. Bile is a digestive fluid that helps the body absorb fat. Gallstones tend to run in families. In addition, high levels of estrogen, insulin, or cholesterol can increase a person's risk of developing them. Pregnancy or the use of birth control pills can slow down gallbladder activity and increase the risk of gallstones. So can diabetes, pancreatitis, and celiac disease. Other factors influencing gallstone formation are: Infection, obesity intestinal disorders coronary artery disease or other recent illness multiple pregnancies a high-fat, low-fiber diet smoking heavy drinking rapid weight loss Gallbladder attacks usually follow a meal of rich, high-fat foods. The attacks often occur in the middle of the night, sometimes waking the patient with intense pain that ends in a visit to the emergency room. The pain of a gallbladder attack begins in the abdomen and may radiate to the chest, back, or the area between the shoulders. Other symptoms of gallstones include: inability to digest fatty foods low-grade fever chills and sweating nausea and vomiting indigestion gas belching. clay-colored bowel movements Gallstones may be diagnosed by a family doctor, a specialist in digestive problems (a gastroenterologist), or a specialist in internal medicine. The doctor will first examine the patient's skin for signs of jaundice and feel (palpate) the abdomen for soreness or swelling. After the basic physical examination, the doctor will order blood counts or blood chemistry tests to detect evidence of bile duct obstruction and to rule out other illnesses that cause fever and pain, including stomach ulcers, appendicitis, and heart attacks. More sophisticated procedures used to diagnose gallstones include: Ultrasound imaging. Ultrasound has an accuracy rate of 96%. Cholecystography (cholecystogram, gallbladder series, gallbladder x ray). This type of study shows how the gallbladder contracts after the patient has eaten a high-fat meal. Fluoroscopy. This imaging technique allows the doctor to distinguish between jaundice caused by pancreatic cancer and jaundice caused by gallbladder or bile duct disorders. Endoscopy (ERCP). ERCP uses a special dye to outline the pancreatic and common bile ducts and locate the position of the gallstones. Radioisotopic scan. This technique reveals blockage of the cystic duct. Watchful waiting One-third of all patients with gallstones never experience a second attack. For this reason many doctors advise watchful waiting after the first episode. Reducing the amount of fat in the diet or following a sensible plan of gradual weight loss may be the only treatments required for occasional mild attacks. A patient diagnosed with gallstones may be able to manage more troublesome episodes by: applying heat to the affected area resting and taking occasional sips of water using non-prescription forms of acetaminophen (Tylenol or Anacin-3) A doctor should be notified if pain intensifies or lasts for more than three hours; if the patient's fever rises above 101°F (38.3°C); or if the skin or whites of the eyes turn yellow. Surgical removal of the gallbladder (cholecystectomy) is the most common conventional treatment for recurrent attacks. Laparoscopic surgery, the technique most widely used, is a safe, effective procedure that involves less pain and a shorter recovery period than traditional open surgery. In this technique, the doctor makes a small cut (incision) in the patient's abdomen and removes the gallbladder through a long tube called a laparoscope. LITHOTRIPSY Shock wave therapy (lithotripsy) uses high-frequency sound waves to break up the gallstones. The patient can then take bile salts to dissolve the fragments. Bile salt tablets are sometimes prescribed without lithotripsy to dissolve stones composed of cholesterol by raising the level of bile acids in the gallbladder. This approach requires long-term treatment, since it may take months or years for this method to dissolve a sizeable stone. CO NTACT DISSOLUTION Contact dissolution can destroy gallstones in a matter of hours. This minimally invasive procedure involves using a tube (catheter) inserted into the abdomen to inject medication directly into the gallbladder. Alternative therapies, like non-surgical treatments, may provide temporary relief of gallstone symptoms. Alternative approaches to the symptoms of gallbladder disorders include homeopathy, Chinese traditional herbal medicine, and acupuncture. Dietary changes may also help relieve the symptoms of gallstones. Since gallstones seem to develop more often in people who are obese, eating a balanced diet, exercising, and losing weight may help keep gallstones from forming. Forty percent of all patients with gallstones have "silent gallstones" that produce no symptoms. Silent stones, discovered only when their presence is indicated by tests performed to diagnose other symptoms, do not require treatment. Gallstone problems that require treatment can be surgically corrected. Although most patients recover, some develop infections that must be treated with antibiotics. In rare instances, severe inflammation can cause the gallbladder to burst. The resulting infection can be fatal.
Add Plop Plop sound bite GERD is the acronym for gastroesophageal reflux disease, a condition in which stomach acid frequently splashes into the esophagus. GERD occurs when the valve connecting the stomach and esophagus becomes weak, turning the junction into a two-way street. Because the esophagus isn't well equipped to handle such a harsh liquid, GERD often causes burning pain and discomfort. Over time, it can even inflict lasting damage. According to the National Institutes of Health, 60 million Americans have symptoms of GERD at least once a month. That includes former Baltimore Orioles Hall of Fame pitcher Jim Palmer, who has said the disease affected his pitching performance. When researchers compared the answers of GERD patients to those of people with other illnesses, they found that some have a worse quality of life than patients with menopausal symptoms, peptic ulcers, angina, or congestive heart failure. If you're suffering from symptoms of GERD, don't ignore the problem. With a few lifestyle changes and a little help from your doctor, you can keep the acid where it belongs. What are the symptoms of GERD? Most people with GERD have frequent bouts of heartburn, typically a tight, burning pain behind the breastbone that moves up towards the neck. The pain usually flares up after meals (especially large meals) and lasts for as long as two hours. Acid regurgitation is another very common symptom of GERD. This occurs when acid travels all the way to your throat, leaving a sour, bitter taste. Heartburn and acid regurgitation are the hallmarks of GERD. If you frequently suffer from either of these symptoms, your doctor can confidently diagnose GERD and move ahead with treatment. Some patients, however, have unusual symptoms that make diagnosis less certain. You may salivate more often than normal, have trouble swallowing, or feel like you have a lump in your throat. In such cases, your doctor may have to run tests to find the source of the problem. What causes GERD? Many different factors can weaken the valve between the stomach and the esophagus, setting the stage for GERD. Food is a common culprit. According to the NIH, fried or fatty foods, chocolate, peppermint, alcohol, and coffee can all lead to GERD. You can open up the floodgates even more by smoking cigarettes. The condition is also common in people who are obese or pregnant. Many patients with severe GERD also have a hiatal hernia, a condition is which a small portion of the stomach pokes through a hole in the diaphragm. In theory, the hernia may weaken the valve between the stomach as the esophagus. However, most people with hiatal hernias don't have GERD. Is GERD serious? Relief from heartburn isn't the only reason to take GERD seriously. Over time, acid can eat away at the lining of the esophagus, causing painful ulcers and even bleeding. This condition is called esophagitis. In a few people, the esophagus protects itself by producing cells that closely resemble cells from the intestine. This is called Barrett's esophagus. Barrett's esophagus, in turn, raises the risk of cancer of the esophagus. If you have Barrett's esophagus, your doctor will want to examine you regularly for signs of dysplasia, a precursor to cancer. This is done by surveying the area through endoscopy, in which a doctor slides a thin tube with a tiny camera at the end down the throat to take pictures and biopsy samples. What can I do to control GERD? A few simple lifestyles changes -- perhaps combined with a couple of not-so-simple changes -- often bring great relief from GERD. Even if your case is severe, a little self-help can go a long way. First, the simple things: Avoid foods that cause symptoms of digestive distress. Foods that often cause symptoms include fatty foods, chocolate, caffeinated food and drinks, citrus fruit or juices, tomato-based products, alcohol, and spicy foods. Eat small meals rather than large ones, and don't lie down within three hours of a meal. If heartburn bothers you at night, try raising the head of the bed six inches, perhaps by sliding blocks of wood under the bedposts. (Putting an extra pillow under your head probably won't help, and can even aggravate the condition.) Some people may need to make more serious changes to their lives. If you're a heavy drinker, GERD is a sign that it's time to cut back. If you smoke, do whatever it takes to quit. If you're overweight, shedding a few pounds could make a big difference. According to Gary Gitnick, MD, chief of the division of digestive diseases at the University of California at Los Angeles School of Medicine, getting 30 minutes a day of exercise can help greatly. (In his book, Freedom from Digestive Distress, Gitnick explains that it's not known why exercise promotes normal digestive function.) Just make sure you go easy on activities that involve bouncing or jumping; they can aggravate your condition. Of course, these steps come with rewards that go far beyond treating your digestive distress. Should I try over-the-counter remedies? When GERD does flare up, an antacid usually brings quick relief. But such relief alone is often not long-lasting. Antacids work best when taken at the first sign of symptoms. Over time, however, regular doses of antacids can cause diarrhea and other side effects. To prevent future attacks -- and break your antacid habit -- you can try an over-the-counter acid blocker such as Pepcid AD, Tagamet, Zantac, or Axid. Ideally, you should talk to your doctor before trying any of these remedies. If GERD is still a problem after two weeks of self-treatment, don't put off that appointment any longer. What kind of tests will my doctor run? If you have the classic symptoms of GERD -- frequent heartburn or acid regurgitation -- your doctor probably won't have to run any tests at all. But if there's any doubt about the cause of your symptoms, your doctor may conduct a barium x-ray or other test to confirm GERD. If you're over 50 and have had GERD for several years, your doctor may use an endoscope to check for Barrett's esophagus. If you have "red flag" symptoms such as dysphagia (difficulty swallowing), progressive weight loss, anemia, or recurrent nausea and vomiting, you should seek medical attention immediately. What is the treatment for GERD? The first line of defense is changing your diet and initiating some of the lifestyle changes suggested above. But if those things don't help or fail to provide enough relief, your doctor can offer several effective treatments. One option is a prescription strength version of Zantac or other acid blocker. More severe cases usually call for drugs known as "proton-pump inhibitors" that strongly block the production of acid. Pill for pill, these drugs are more expensive than standard acid blockers. But if you have severe GERD, proton-pump inhibitors may be cheaper in the long run because it takes fewer pills to bring relief and because they help heal ulcers in the esophagus. Prescription drugs for GERD are generally safe and easy to take. A few patients develop headaches or diarrhea. Less common side effects include nausea, gas, abdominal pain, constipation, and dry mouth. If medications fail to control your heartburn, or if your symptoms come roaring back as soon as you stop taking medications, surgery may be your best chance for long-term relief. Surgery may also be necessary if you have formidable damage to your esophagus, severe esophagitis, Barrett's esophagus, or other complications. Surgery, however, should be a last resort after all other treatments have failed.
![Objectives ,[object Object],[object Object],[object Object],[object Object]](data:image/gif;base64,R0lGODlhAQABAIAAAAAAAP///yH5BAEAAAAALAAAAAABAAEAAAIBRAA7)