MOSQUITO-BORNE JAPANESE ENCEPHALITIS
•Descargar como PPTX, PDF•
0 recomendaciones•249 vistas

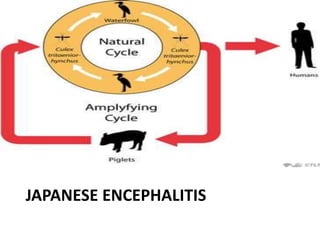
This document summarizes information about Japanese encephalitis (JE), including: - JE is a mosquito-borne viral disease that causes brain inflammation and is a major public health problem in Asia. - It is transmitted by Culex mosquitoes and has pigs and wading birds as amplifying hosts. - Up to 50,000 cases and 10,000-15,000 deaths are reported each year globally. Many survivors are left with long-term disabilities. - Control relies on surveillance of cases and vectors, vaccination programs, and reducing mosquito breeding sites.

Recomendados
Más contenido relacionado
La actualidad más candente
La actualidad más candente (20)
Similar a MOSQUITO-BORNE JAPANESE ENCEPHALITIS
Similar a MOSQUITO-BORNE JAPANESE ENCEPHALITIS (20)
Más de Siva Mbbs
Último
Último (20)
MOSQUITO-BORNE JAPANESE ENCEPHALITIS
- 2. • mosquito-borne encephalitis caused by a group B arbovirus (Flavivirus) and transmitted by Culicine mosquitoes • More than 3 billion people live in areas where JE is transmitted. • Up to 50,000 cases of JE are reported to WHO each year. • Up to 10,000 to 15,000 deaths are reported each year. • nearly 15,000 disabled
- 3. Why is JE a problem? • JE is the leading cause of viral neurological disease in Asia, now that poliomyelitis has nearly been eradicated. • case fatality rate 20-40 % • For those that survive the illness, 30% to 75% cases are left with disability. • Disability is both physical and cognitive. Epidemic potential , high case fatality and life long sequelae
- 4. Animal Hosts • mainly include pigs and water birds e.g. pond herons, cattle egrets, poultry birds and ducks • studies of the presence of JE antibodies in the sera of birds have indicated that Ardeola grayii (pond heron) and Bubulcus ibis (cattle egret) play a definite role in maintenance of JE virus in nature
- 7. • Pigs act as amplifying hosts • Cattle and buffaloes –mosquito attractants-no role in transmission • Man-incidental host
- 8. VECTORS • C.tritaeniorhynhus,C vishnui ,C.pseudovishnui and C.gelidus • Breed in irrigated rice fields,pools and ditches • Mosquitoes are zoophilic • Epidemics usually coincide with monsoons and post- monsoon period when the vector density is high. • extrinsic incubation period of 9 to 12 days. • mosquitoes remain infected for life. The average life period of a mosquito is about 21 days. Culex mosquito can fl y for long distances (1-3 kms. or even more).
- 9. • Principal vector in kerala • Mansonia annulifera, Mansonia uniformis and Mansonia indiana- 'bridge vector' of JE in Kuttanadu area where these mosquitoes are abundant. C.tritaeniorhynchus
- 11. Clinical manifestations • incubation period in man- 5 to 15 days. • Only 1 in 250–500 JE viral infections are symptomatic. • JE manifestations divided into • A Prodromal Stage • An Acute encephalitic Stage • and a late stage
- 12. Prodromal Stage : • Fever • malaise • Rigors • Headache • Nausea • and Vomiting • The Prodromal stage usually lasts for 1 to 6 days.
- 13. An Acute Encephalitic Stage: Begins by the third to fifth day. The symptoms include: • Convulsions • Altered sensorium, unconsciousness, coma • Stiff Neck • Muscular Rigidity • Tremors in fingers, tongue, eyelids and eyes. • Abnormal movements of limbs • Speech impairment
- 14. A Late Stage: Characterised by • Improvement/the persistance of signs of CNS injury such as • Mental impairment. • Increased deep Tendon reflexes • Paresis either of the upper or lower motor neuron type. • speech impairment • Epilepsy, Abnormal movements, Behaviour abnormalities.
- 15. Laboratory diagnosis • IgM antibodies appear after the first week of onset of symptoms and are detectable for one to three months • A four fold rise in IgG antibody titre in paired sera taken at an interval of 10 days or more is confi rmatory. • Virus isolation from brain tissue • Antigen detection by immunofluroscence • Nucleic acid detection by PCR
- 16. treatment 1.) Management of Airways and Breathing. 2.) Management of Circulation. 3.) Control of Convulsion and Intracranial pressure 4.) Control of Temperature 5.) Fluid and Electrolytes and Calories/ Nutrition 6.) General management 7.) Specific treatment of any for treatable cause 8.) Investigations, Samples Collection 9.) Reporting of a case 10.) Rehabilitation.
- 17. JE CONTROL STRATEGY • Early Case Detection and Treatment • Vector Control a)reduction of breeding source for larvae b) reduction in man-mosquito contact c) control of adult mosquitoes • Prevention a) je vaccination • Surveillance
- 18. Prevention & Control • Reservoir Control • Surveillance • Early case detection and treatment • Interruption of Transmission – Vector Control • Protecting host - Vaccination
- 19. Objectives of JE Surveillance • Detect early warnings signals • Strengthen lab services • Assess impact of vaccination
- 20. Strategies of JE Surveillance • Epidemiological Surveillance for AES • Entomological Surveillance • Veterinary based Surveillance
- 21. Epidemiological Surveillance for AES Case Definition of AES • A person of any age, at any time of the year with acute onset of fever and a change in mental status (including confusion, disorientation, inability to talk or coma) and/ or new onset of seizures (excluding simple febrile seizures).
- 22. Suspected JE (AES) Adequate blood/CSF IGM -ve Other diagnostic test AES – other agent AES unknown IGM +ve Lab confirmed JE No adequate blood/CSF Geographical/temp link to lab confirmed Probable JE No geographical/temporal link AES unknown
- 23. Case Classification A case that meets the clinical case definition for AES – classified in one of the four ways Laboratory confirmed JE: A suspected case that has been laboratory confirmed as JE Probable JE: A suspected case that occurs in close geographic and temporal relationship to a laboratory confirmed case of JE, in the context of an outbreak.
- 24. Case Classification Acute Encephalitis Syndrome (due to other agent) – A suspected case in which diagnostic testing is done & an etiological agent other than JE is confirmed Acute Encephalitis Syndrome (due to unknown agent) – A suspected case in which no diagnostic testing is performed or in which diagnostic testing is performed but no etiological agent was identified or in which the test result was indeterminate
- 25. Implementation of JE / AES Surveillance • Sentinel Surveillance Sites with Laboratories facilities. (SSSL) • Sentinel Surveillance Sites without laboratories facilities.(SSS without Lab.) • Other Informer Units.
- 26. Sentinel Surveillance Sites with Laboratories facilities. (SSSL) • Tertiary care hospital – MC, Regional, DH • Nodal Officer -> District Malaria Officer • Records and report – maintain documentation SSSL - JEF3, JEF4, JEF5 • Monthly basis – Inter epidemic period • Weekly basis – transmission season • Daily basis – during outbreak
- 27. Sentinel Surveillance Sites without laboratories facilities (SSS without Lab.) • DH, CHC, PHC • Linked with nearest SSSL • Linelist of AES case / Record of JE maintained • Submitted to DMO / State Programme Officer • Format – JEF3 & JEF4 • Frequency – Daily , weekly & monthly to DMO
- 28. Other Informer Units. • Smaller health facility , private practioners • Inform DMO / SMO • Do not maintain detailed documentation of patients. • AFP surveillance network
- 29. JE Surveillance Activities – District Level • DMO – study & monitor the daily/weekly/monthly/nil reports from all units • Reconcile data with IDSP – forward to SPO(senior programme officer) • Compile all reports - interpretation and action. • Supervision & monitoring of all levels.
- 30. 1. Case Investigation a) Verification of case definition – personally see the case and discuss with reporting physician. b) Patient code number assigned – 11 alphabet with seven digit numerical code(IND-AESUP-XXX-01-001) c) JEF4 – history,conduct the physical examination, fill JEF5 and AES case identification, coordinate collection of serum and CSF specimen.
- 31. 2. . Visit to Sentinel Surveillance Sites • Meet the Nodal Officer • Visit IP / OP – scan the registers • Identify training needs
- 32. 3. Visit to AES Informers • Regular visit by DMO / SPO • Monitor surveillance activity • Sensitize the staff • Update informers on the importance of AES reporting
- 33. Surveillance activities at State level • All reports from the district is merged and collated • Transmit to director, NVBDCP in JEF1 & JEF1A forms. • Daily reporting –> JEF1A • Take rapid action for containment
- 35. Process of AES Surveillance Febrile illness with altered sensorium Detection & notification Case investigation Specimens arrive Serological blood & CSF collection at laboratory results Line listing Classification of isolated cases Implications of control measures Data analysis & interpretation Compile JE outbreak Investigation report
- 36. Surveillance activities - National • Data from districts compiled - national report with epidemiological inferences • Data shared with international organisation • Report – basis for planning , containment activities and allocation of resources
- 37. Entomological Surveillance • To identify JE vector mosquitoes in the area • To monitor the vector abundance • To detect JE virus in vector • To suggest appropriate vector control measures.
- 38. Procedure of entomological surveillance • Index village selected – 3 JE occurred in the recent past + 2 unaffected will be monitored • Sampling carried out on fortnightly basis • Surveillance carried out round the year – JE vector density, feeding & resting behaviuor – detection and isolation of virus from vector
- 39. Veterinary based surveillance Objectives • Prevalence of Pigs / Ducks, Ardeid Birds in an area • To Detect viral Activity in susceptible hosts Animal Husbandry Dept. • Pigs – antibody titer – viral activity • 5 – 8 month old piglets blood samples – IgM antibody – recent infection
- 40. Vector Control Indoor residual spray Fogging Personal protective measures Anti larval operations Reduction of breeding source of larvae Larvivorous fish Biolarvicides Reduction in man vector contact
- 41. Control of Pigs • Immunisation • Slaughtering • Use of mosquito proof piggeries • Segregating pigs 4-5 km away
- 42. Behavior Change Communication Imparted through all probable approaches Personal prophylaxis against vector Segregation of amplifier host Early reporting of cases
- 43. JE Vaccination 3 Types of vaccines o Inactivated mouse brain o Inactivated primary hamster kidney cells o Live attenuated SA-14-14-2 – single dose, s/c
- 44. JE Vaccination Strategy-India • One time mass campaign in 1-15yrs in endemic districts • Integrate into routine immunisation to cover new cohort along with DPT booster • Coverage both urban & rural children • 2008 –Alappuzha – 42 % • 2009 – Thiruvananthapuram- 39 %
- 45. Criteria to identify district • Case load of JE • Incidence of JE • Evidence of recent transmission • Serological evidence fom studies • Epidemiological link to known areas of transmission
- 46. THANK YOU