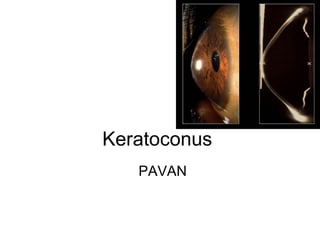
2. DEFINITION
• Progressive,
• Non inflammatory,
• Bilateral (usually asymmetrical)
• Cone like anterior protrusion of the
cornea involving the central and the
inferior paracentral areas that results in
corneal ectasia, astigmatism, & decreased
vision.
• Incidence of 1 in 2000 of general
population.
DOS Times - Vol. 15, No. 10, April 2010
3. • Usually seen after puberty
• No gender predominance
• No race predominance
• The patient becomes myopic but the error
of refraction cannot be satisfactorily
corrected with ordinary glasses owing to
parabolic nature of the curvature which
leads to irregular astigmatism.
4. • sub clinical keratoconus is seen in family
members or the fellow eye.
• No frank clinical sign
• The cornea is at risk of developing
keratoconus at a later stage and can be
diagnosed only by videokeratography.
DOS Times - Vol.10, No. 7 January 2005
5. • Classifaication BY krumeich based on astigmatism, & thichness..
• Stage 1: Eccentric corneal steapening
• induced myopia or astigmatism -5D
• corneal radii 48D
• Vogts sriae, no scar
• Stage 2:
• induced myopia or astigmatism -5D to -8D
• corneal radii 48D
• Vogts sriae, no scar
• Corneal thickness 400 ums
• stage 3: induced myopia or astigmatism -8D to-10D
• corneal radii 53D
• Vogts sriae, no scar
• Corneal thickness 200 to 400 ums
• Stage 4: reraction not measurable
• corneal radii 55D
• corneal scars+, perforations+
• Corneal thickness 200 ums
•
6. • B: Based on keratometry
• mild <48D
• moderate 48 -54D
• severe: >54D
• C: Based on morphology
• nipple cones(central <5mm)
• oval/sagging cones(5-6mm)
• globus cones(>6mm)
7. Etiology
• Various theories:-
• Thinning may be due to
• Defective formation/destruction of extracellular
matrix
• Abnormal collagenase activity.
• Increased levels of proteases &catabolic
enzymes in the basal epithelial cells
• Decreased levels of proteinase inhibitors:
alpha 1 proteinase inhibitor ,
alpha 2 macroglobulin.
8. • Excessive eye rubbing or atopic disease-
• induces keratoconus by inducing
• epithelial damage-----
• epithelial stress----
• increased keratocyte apoptosis through
interluekin 1 causing changes in stomal
matrix
• Hard contact lens wear
• 6-15 % positive family history.
9. • The role of heredity not been clearly
established. .
• In some cases, however,
• a sex-linked
• autosomal dominant mode of inheritance,
particularly because of the predominance
of familial females with keratoconus.
12. Ocular association
• Vernal keratoconjunctivitis
• RP
• Leber’s congenital amaurosis
• Retinopathy of prematurity
• Progressive cone dystrophy
• Aniridia
• Iridoschisis
• Iris atrophy
• Fuchs' dystrophy
• Posterior polymorphous dystrophy
• Granular and lattice dystrophies
13. Histopathology
• Triad of classical histopathologic features
– Thinning of the corneal stroma
– Breaks in Bowman’slayer
– Deposition of iron in the basal layersof the
corneal epithelium
Depending on the stage of the disease,
every layer and tissue of the cornea can
become involved
14. • The epithelium may show degeneration of
its basal cells, breaks accompanied by
down growth of epithelium into Bowman’s
layer
• Accumulation of ferritin particles within
and between epithelial cells most
prominently in the basal layer of the
epithelium.
.
15. • Bowman’s layer may
include breaks
• filled by eruptions of
underlying stromal
collagen, periodic acid
Schiff–positive nodules.
• Z-shaped interruptions,
possibly due to
separation of collagen
bundles and reticular
scarring.
16. • In stroma changes seen are compaction
and loss of arrangement of fibrils in the
anterior stroma
• decrease in the number of collagen
lamellae
• normal and degenerating fibroblasts in
addition to keratocytes,
• fine granular and microfibrillar material
associated with the keratocytes.
17. • Descemet’s membrane is rarely affected
except for breaks seen in acute hydrops.
• The endothelium is usually normal.
However, some abnormalities like
• intracellular “dark structures,”
• pleomorphism, and elongation of cells with
their long axis toward the cone.
18. Symptoms
• Progressive visual blurring and/or distortion
• Rapidly changing spectacle prescription
• Eye rubbing
• Photophobia
• Glare
• Monocular diplopia
• Sudden onset of pain, redness, loss of
vision, and photophobia suggests hydrops
19. • The onset of keratoconus occurs
predominantly in the late teens.
• Symptoms usually appear bilaterally, but
asymmetric presentation.
• During the first 5-7 years of onset, the
condition generally worsens with
intermittent periods of remissions
20. SIGNS KKKKKK
• Munson’s sign is a V-shaped conformation of the lower
lid produced by the ectatic cornea in downgaze.
• Rizzuti’s sign is a sharply focused beam of light near
the nasal limbus, produced by lateral illumination ofthe
cornea in patients with advanced keratoconus.
• Charleux”s sign: Dark reflex in the centre of cornea
with DDO in dilated pupils..
• Pulsations of mires on applanation tonometry
• Pulsations of reflected images in keratometry.
22. Slit lamp examination
• Fleischer's Ring
– The Fleischer ring is a
yellow-brown to olive-
green ring of pigment
which may or may not
completely surround
the base of the cone
– Formed when
hemosiderin (iron)
pigment is deposited
deep in the epithelium
– Fleischer's ring often
becomes thinner and
more discrete with
progression
23. • seen approximately 50% of all cases.
• Locating this ring initially may be made
easier by using a cobalt filter and carefully
focusing on the superior half of the
cornea's epithelium.
• Imp : gives information about extent of
ectasia, which helps during surgery &
prognosis after P.K..
24. Lines of Vogt
• small and brushlike lines, generally vertical but they can
be oblique.
• Found in the deep layers of the stroma and form along
the meridian of greatest curvature.
• Disappear when gentle pressure is exerted on the globe
through the lid.
25.
26. Corneal Thinning:
• Significant thinning (up to 1/5th cornea
thickness) in the advanced stages of the disease
and
• A diagnostic criterion based on comparison of
central and peripheral corneal thickness has
been proposed.
• Additionally, as the disease progresses, the
cone is often displaced inferiorly.
• The steepest part of the cornea (apex) is
generally the thinnest.
27.
28. Corneal Scarring
• Sub-epithelial corneal
scarring, not generally
seen early, may occur as
keratoconus progresses
because of ruptures in
Bowman's membrane
which is then filled with
connective tissue
• Deep opacity of the
cornea are also common
in keratoconus.
29. Corneal Hydrops:
• Corneal hydrops occurs in advanced cases,
• when Descemet's membrane ruptures, aqueous flows
into the cornea and reseals
• Keratoconus patients who are having an acute episode
of corneal hydrops report a sudden loss of vision and a
visible white spot on the cornea.
• Corneal hydrops causes edema and opacification.
30. • As Descemet's regenerates, edema and
opacification diminish.
• Occasionally, hydrops can benefit keratoconus
patients who have extremely steep corneas.
• If the cornea scars, a flatter cornea often
results, making it easier to fit with a contact lens.
• An increased incidence of hydrops has also
been reported in keratoconus patients with
Down's syndrome.
31.
32. Diagnosis
• Early keratoconus usually manifests as a small
island of irregular astigmatism in the inferior
paracentral cornea.
• As the cornea bulges outward, the amount of
astigmatism increases due to the progressive
distortion of the corneal surface.
• These changes can easily be seen as irregular
mires on keratometry readings and on
corneal topography, a test used to map the
topographical surface area of the cornea
33. • Many objective signs are present in
keratoconus.
• Retinoscopy shows a scissoring reflex.
• Direct ophthalmoscopy may show a
shadow If the pupil is dilated and a +6.00
D lens is in the ophthalmoscopic system,
the cone may appear as an oil or honey
droplet when the red reflex is observed-
Charleux” oil droplet sign
34. • The photokeratoscope or topographer
placido disc can provide an overview of
the cornea and can show the relative
steepness of any corneal area.
• The even separation of the rings in the
spherical cornea ".
36. • In astigmatic cornea uneven spacing of
the rings--especially inferiorly--in the
keratoconic cornea should be noted
• . The central rings may show a tear-drop
configuration termed "keratokyphosis".
37. • The keratometer also aids diagnosis.
• The initial keratometric sign of
keratoconus is absence of parallelism and
inclination of the mires. These can easily
be missed in mild or early cases.
38.
39. Rabinovitz criteria for diagnosis
of keratoconus
1. Central corneal power >47.2D
2. Inferior superior dioptric assymetry over
1.2
3. Sim K astimatism >1.5D
4. Skewed radial axes more than 21
degrees
40. Corneal topography
• Provides a color coded map of the corneal
surface.
• The power in diopters of the steepest and
flattest meridians and their axes are
calculated and displayed
• Steep curvatures are marked orange or
red
• Flat curvature in blue or violet
• Normal curvatures in green or yellow
41. Classification scheme of normal videokeratographs
in the absolute scale devised as a baseline to monitor
topographic progression to keratoconus A, round:
B, oval: C, superior steepening; D, inferior steepening; E,
irregular; F, symmetric bow tie; G, symmetric bow tie with
skewed radial axes; H, asymmetric bow tie with inferior
steepening (AB/IS); I, asymmetric bow tie with superior
steepening; J, asymmetric bow tie with skewed radial axes
(AB/SRAX
42. • Two figures are a schematic
illustration of how to determine
whether a pattern is AB/IS or AB/
SRAX.
• A line is drawn to bisect the upper
and lower lobes of the asymmetric
bow tie,
• If there is no significant deviation
from the vertical meridian (i.e., no
skewing), the pattern is
designated as AB/IS (as in A);
• if the lines bisecting the two lobes
appear skewed by more than 21
degree from the vertical meridian
(i.e., 150 deg from one another), it
is labeled as AB/SRAX (as in
Bottom B).
44. Corneal topography
• Rabinowitz developed algorithms for detection of
keratoconus based on 3 observations
• Diopteric power difference between the sup and
inf paracentral cornea I/S >1.9
• Central corneal power >48.7 D
• Difference in progression of corneal steepening
between two eyes
• Method yeilds positive result In case of
keratoconus suspect-
• if I/S value is >1.4 and central corneal power
>47.2D.
45. INDICES
• SIM-K (MAX &MIN)
• APICAL POWER
• ASTIGMATIC INDEX
• IRREGULARITY INDEX
• ANTERIOR ELEVATION
• POSTERIOR ELEVATION
• INF –SUP ASYMETRY
46. • SIMULATED K READINGS:
• Corneal curvature In the central 3 mm area
• Steep sim-k reading in 3 mm indicates steepest
meridian, & flattest will be 90* apart to this.
• SURFACE ASSYMETRY INDEX:
• Indicates changes in curvature of cornea from
centre to peryphery,
• Normally cornea is prolate, with ashperycity-
0.26, but in K.C it becomes oblate with positive
aspherycity value
47. • IRREGULARITY MAP: it displays the
distortions of cornea using previous
elevation map, & represents with hot
colours…
• ANTERIOR ELEVATION:
• with BFS: to locate the cone
• WITH BFTE(best fit torric ellipsoid): to
check the real height of the cone
• Red indicates raised, & blue flat.
48. normal K.C suspect K.C
Central k
reading
44.17 45.13 48.97
I-S assyemtry 0.57 1.20 4.4
49. KISA INDEX
• INCLUDES FOUR COMPONENTS
• K READINGS
• I-S ASSYMETRY
• ASTIGMATISM INDEX
• SRAX
• KISA=K x I-S x AST x SRAX x 1/3
• 100% =KERATOKONUS
• 60-100% =SUSPECT
• <60% = NORMAL
53. Spectacles
• Mild keratoconus can be corrected with
spectacles.
• Retinoscopy is difficult;
• a normal subjective refraction is required.
• Monocular keratoconus is usually best
dealt with using spectacle correction.
55. Contact lenses
• Contact lenses are considered when vision is
not correctible to 6/9 by spectacles and patients
become symptomatic.
• Rigid gas permeable (RGP) corneal lenses are
the lenses of first choice.
• The aim is to provide the best vision possible
with the maximum comfort so that the lenses
can be worn for a long period of time.
56.
57.
58.
59. • Based on shape of cone
• Nipple cone : small diameter (5 mm.); round
shape; easiest to fit with contact lenses
• Oval large diameter(>5 mm.); often displaced
inferiorly; more difficult to fit with lenses
• Globus largest diameter (>6 mm.); 75% of
cornea affected; most difficult to fit with lens
61. Fitting methods
• 1) Three-point-touch design
• Contact at the central apical area & two
horizontal mid periphery area at 3 & 9’ -0 clock
position.
• The three-point-touch design is the most popular
and the most widely fitted design
• The aim is to distribute the weight of the contact
lens as evenly as possible, between the cone
and the peripheral cornea.
62. • The ideal fit should show an apical contact
area of 2-3mm with mid-peripheral
contact.
• Adequate edge clearance is required to
ensure tear exchange.
63.
64. 2) Apical clearance
• In this type of fitting technique:
• the lens vaults the cone and clears the central
cornea, resting on the paracentral cornea.
• These lenses tend to be small in diameter and
have small optic zones
• The potential advantages of reducing central
corneal scarring are outweighed by the
disadvantages like poor tear film, corneal
oedema, and poor visual acuity as a result of
bubbles becoming trapped under the lens.
65.
66. • 3) Flat fitting
• The flat fitting method places almost the entire weight of
the lens on the cone.
• The lens tends to be held in position by the top lid.
• Good visual acuity is obtained as a result of apical touch.
• Alignment can be obtained in early keratoconus;
• however, flat fitting lenses can lead to:
- progression/ acceleration of apical changes and
corneal abrasions.
• This type of fitting is useful where the apex of the cone is
displaced.
67.
68.
69.
70.
71.
72.
73. • Piggy back lenses can be used in pts who are
uncomfortable with RGP wear.
• And in pts who are more prone to epithelial
erosion at apex of cone.
74. ROSE-K
• Introduved by Paul rose, & k means keratoconus .
• specially designed for kearatoconic eyes with a
diagnostic set of 26 lenses with base curves ranging
from 5.1 to 7.6 mm in 0.1 increments,
• A std lens diameter is 8.7mm.
• Features .
• Customized complex geometry suitable in correcting
high myopia & astigmatism.
• Easy to insert & remove.
• Provide excellent health to eye.
• Good oxygen permeability.
75. • Rose –k lenses have more curves on back surface of
lens, in such a way that adjacent curves are very
different from each other,
• Causes different focal points for each curve
• Leads to more aberrations
• To overcome this problem he introduced rose –k2 lenses
in 1998, which are having small changes in curves in
both front & back surface of the lens
76.
77. Soper lens
Custom made lens
Two zones in the posterior curvature.
Central zone : to vault steep central
cornea .It is of varying steepness
depending of the patients cornea.
Peripheral zone is with a 45D curvature
designed to vault the mid periphery and
limbal cornea
79. Scleral lenses
• Scleral lenses play a very significant role
in cases of advanced keratoconus where
corneal lenses do not work and corneal
surgery is contra-indicated.
• Scleral lenses completely neutralise any
corneal irregularity and can help patients
maintain a normal quality of life
80. Boston scleral lens prosthetic
device (BSLPD)
• Fluid ventilated scleral lens
• Designed to enclose a bubble free
reservoir of fluid over the corneal surface
• Series of breaches are created between
haptic bearing surface of the lens and
underlying sclera.
81. • This will facilitate the aspiration of surface
tears into the reservoir so that intrusion of
air bubble during a blink is prevented.
• Shape of haptic confirms exactly to that of
underlying sclera to maintain functionality
and prevents intrusion of air bubbles.
• Very expensive
82.
83. Collagen cross linking by
riboflavin and UVA
• Photopolymerisation of collagen fibers by
photosensitizing substance like(riboflavin
or vit b2)+uv type a rays from a solid state
UV source
84. • Indications
– Progressive keratoconus
– Eyes with mild to moderate keratoconus
– Corneal thickness > 400 µm
– No slit-lamp evidence of corneal scarring
– Preferably age < 35 yrs since complication rate
increases after 35yrs
85. Combining UV radiation and riboflavin is the most
effective method to induce collagen cross linking.
86. STEPS
• Using topical anaesthesia,
• 7mm circle is marked on the cornea using a
marker.
• Epithelium of the marked area is scraped off
using a blunt spatula.
• A corneal abrasion is created to facilitate
riboflavin diffusion into the cornea.
87. • One drop of riboflavin 0.1% and 20%
dextran ophthalmic solution is instilled
topically in the eye every 2 minutes for 30
minutes.
• After 30-minute, the eye is examined
with blue light for the presence of a yellow
flare in the anterior chamber, indicating
adequate riboflavin saturation of the
corneal tissue.
88. • When the yellow flare in the anterior chamber is
confirmed,
• the eye is aligned under the UV-A light .
• Focussed on the apex of cornea at a distance of 10-12m
to obtain a radiant energy of 5.4J/cm2 for 5 min.
• The correct aperture setting is selected for the size of the
eye;
• the eye is irradiated for 30 minutes, during which time
instillation of riboflavin is continued (one drop every 5
minutes).
89. Issue: February 2009
Collagen Cross-linking
What you should know about this potential new
treatment for keratoconus and ectasia.
BY YARON S. RABINOWITZ, M.D.
90. • After completion of the procedure,eye is
washed with BSS , an antibiotic drop is
instilled and a bandage contact lens is
applied.
• The contact lens is removed once the
abrasion has healed.
• Postoperative medications include an
antibiotic and a steroid for 2 weeks
postoperatively.
91. • There are reports of the procedure being performed
without removing the epithelium.
• This is attractive to patients since they would forgo the
pain caused by the abrasion, as well as decrease their
risk for infection due to an open wound.
• Bottos et al. demonstrated that the epithelium is a barrier
to crosslinking and very little cross-linking occurs in the
presence of epithelium showed by immunofluorescent
confocal microscopy studies.
• These findings suggest that for the treatment to be
effective, the epithelium should always be removed
92. Results
• The procedure appears to be relatively safe.
• The only adverse event reported to date after cross-
linking has been corneal edema in an eye with a
pretreatment corneal thickness of less than 400 microns,
presumably caused by UV damage to the corneal
endothelium
• Subsequent experiments led to the conservative
recommendation that corneas not be treated with
UVA/riboflavin unless they are thicker than 400 microns
after epithelial debridement. Thus preop pachy is very
imp.
• Other complications reported in the literature are a case
of HSV keratitis and DLK in a case of post-LASIK
ectasia. Both resolved without any long term-effects on
the patients
Ophthalmology Management Issue: February 2009
Collagen Cross-linking - potential new treatment for keratoconus
and ectasia.
BY YARON S. RABINOWITZ, M.D.
94. Intracorneal stromal rings
• Act as passive spacing agents which flatten the
cornea
• Made of PMMA
• Amount of correction depends on the ring
thickness,more thicker the ring more correction.
• On insertion they shorten the arc of ant corneal
surface,iron out gross irregularities and in effect
create a second limbus.
• Various corneal ring- Ferarings, intacs.
95. • An important potential benefit of treating keratoconus
with INTACS inserts is to delay or eliminate the need for
a corneal graft.
• Patients with mild to moderate keratoconus appear to be
the best candidates.
• Thickeness varies from 0.21mm to 0.45mm
-Selection of intacs depends on ::
-Pre op manifest refraction
-Location of cone
-Amount of astigmatism
-Spherical eqvivalent
96. INDICATIONS
• This procedure is good for patients:
– contact lens intolerant
– Whose central cornea is clear
– K readings are not in excess of 58 Diopters
– > 400 microns
– To Patient where only corneal transplantation is
the remaining option.
97. • under topical anesthesia,
• a small corneal incision (1.8 mm in length)
was made temporally at the edge of the 7-
mm optical zone
• Two intrastromal tunnels (clockwise and
counterclockwise) were created.
98. • Special care was taken when making the
Inferior tunnel, where the cornea is
relatively thinner.
• a 0.45-mm INTACS insert was placed
inferiorly to lift the conus, and
• a 0.25-mm INTACS insert was placed
superiorly to flatten the cornea and
decrease baseline keratoconic
asymmetric astigmatism.
99. • The selection of segments is based on std
normograms
• In globus or central cone-2 rings of equal
thickness
• Assymetrical cone-thin in flatter and thick
in steeper-usually inferior.
100. • The corneal wound was gently hydrated during
INTACS inserts placement, and edges of the
stroma were approximated to prevent epithelial
ingrowth.
• The incision was closed with one 10–0 nylon
suture.
• A topical antibiotic/steroid combination was
applied postoperatively and a clear shield put on
the eye for recovery.
• The suture was removed 1 to 4 weeks after the
surgery,
101.
102.
103.
104. Complications
of INTACS
• Undercorrection-residual myopia-thicker rings in
steeper area
• Overcorrection-if pt hyperopic thin ring can be
exchanged
• Migration of rings
• Extrusion or progressive thinning
• New vessel formation
• glare /halos
105. Contraindications
• Collagen vascuar diseases
• Autoimmune/immunodeficiency diseases
• Pregnant / nursing mother,
• Ocular conditions such as recuurent
corneal errosion syndromes/dystrophy
• Whose pupillary diameter more than 7mm
• Patients on isoretinoin , sumatriptan,
amiodarone
107. Phakic iols
• Used to correct high myopia and
associated astigmatism of selected
keratoconus patients.
• Anterior chamber phakic intraocular lens
have also been combined with intacs with
good results.
• The INTACS implantation is followed by
toric phakic intraocular lens implantation
to correct the residual myopic and
astigmatic refractive error.
108. PHAKIC IOLS
• INCLUSSION CRITERIA:
• Stable refractive error for more than one year
• Clear central cornea
• Central dioptric power should be less than 52D
• EXCLUSSION CRITERIA:
• Central ant chamber depth less than 2.8mm
• Endothelial cell count less than 2000/mm2
• Patient younger than 21years
109. Penetrating Keratoplasty
• The gold standard surgery
• Success rate is more than 90%.
• In this procedure, the keratoconic cornea
is prepared by removing the central area
of the cornea, and a full-thickness corneal
button is sutured in its place.
• Usually trephines between 8.0-8.5 mm
are used.
110. • Fleischer’s ring can be used as the limit of
the conical cornea.
• Contact lenses are often required after this
procedure for best visual rehabilitation.
111. Anterior deep lamellar
kearatoplasty
• Partial corneal transplant.
• The cornea is removed to the depth of posterior stroma,
and the donor button is sutured in place.
• This technique is technically difficult, and visual acuity is
inferior to that obtained after penetrating keratoplasty.
• As a result, use of lamellar keratoplasty is largely
confined to the treatment of large cones or keratoglobus
when tectonic support is needed.
• This technique requires less recovery time, and poses
less chance for corneal graft rejection or failure.
• Its disadvantages include vascularization and haziness
of the graft
112. Thermokeratoplasty
• Rare procedure
• It involved placing a hot ring (Holmium yag
laser, 2100nm) along the base of the cone
to heat and traumatize the cornea,
resulting in a corneal scar which reduces
the corneal curvature.
• It allows a flatter contact lens to be fitted..
113. • The disadvantages of the procedure
• transitory corneal haze
• development of corneal scarring
DOS Times - Vol. 14, No.1, July 2008
114. • STUDY :Penetrating and Deep Anterior Lamellar
Keratoplasty for Keratoconus: A Comparison of
Graft Outcomes in the United Kingdom
• PURPOSE. To compare outcomes after penetrating
keratoplasty (PK) and deep anterior lamellar keratoplasty
(DALK) for keratoconus in the United Kingdom.
• METHODS. Patient outcome data were collected at the
time of transplantation and at 1, 2, and 5 years after
surgery.
115. RESULTS.
• The risk of graft failure for DALK was almost twice that
for PK
• Nineteen percent of the DALK failures occurred in the
first 30 postoperative days compared with only 2% of PK
failures.
• there was little difference between the 3-year graft
survivals for DALK and PK Although the mean best
corrected visual acuity (BCVA) was similar for the two
procedures.
• 33% of patients who underwent PK achieved a BCVA of
6/6 or better at 2 years compared with only 22% of those
who underwent DALK )
• Those with DALK were also likely to be more myopic ( 3
D) but there was little difference in scalar cylinder.
116. • CONCLUSIONS.
• DALK had a higher overall failure rate than PK.
• The difference was largely accounted for by
early failures, which appeared to be related to
the surgeon’s experience.
• DALK recipients were less likely to achieve
BCVA of 6/6 than were PK recipients and were
more likely to have 3 D or worse myopia.
(Invest Ophthalmol Vis Sci. 2009;50:5625–5629)
DOI:10.1167/iovs.09-3994