Osteoporosis is a disease where bone density decreases to the point of potential fracture. It occurs when bone resorption exceeds bone formation, resulting in porous and fragile bones. Key factors that increase the risk include low estrogen after menopause, physical inactivity, glucocorticoid use, and older age. Treatment focuses on preventing further bone loss with bisphosphonates or drugs that inhibit bone resorbing cells like denosumab.
All Time Service Available Call Girls Marine Drive 📳 9820252231 For 18+ VIP C...
Osteoporosis
1. Osteoporosis
Osteo- refers to bones and -porosis means pores.
osteoporosis is when there's a higher breakdown of bone in comparison to the formation
of new bone which results in porous bones, meaning a decrease in bone density to the
point of potential fracture.
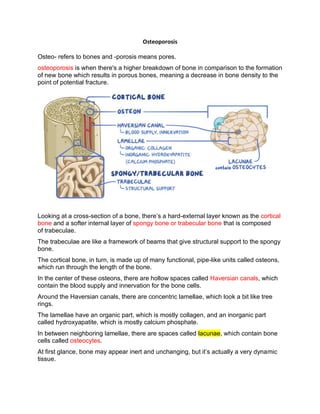
Looking at a cross-section of a bone, there’s a hard-external layer known as the cortical
bone and a softer internal layer of spongy bone or trabecular bone that is composed
of trabeculae.
The trabeculae are like a framework of beams that give structural support to the spongy
bone.
The cortical bone, in turn, is made up of many functional, pipe-like units called osteons,
which run through the length of the bone.
In the center of these osteons, there are hollow spaces called Haversian canals, which
contain the blood supply and innervation for the bone cells.
Around the Haversian canals, there are concentric lamellae, which look a bit like tree
rings.
The lamellae have an organic part, which is mostly collagen, and an inorganic part
called hydroxyapatite, which is mostly calcium phosphate.
In between neighboring lamellae, there are spaces called lacunae, which contain bone
cells called osteocytes.
At first glance, bone may appear inert and unchanging, but it’s actually a very dynamic
tissue.
2. spongy bone is replaced every 3 to 4 years and compact bone is replaced every 10
years, in a process called bone remodeling which has two steps:
- bone resorption when specialized cells called osteoclasts break down bone
- bone formation which is when another type of cells called osteoblasts form new
bone.
Bone remodelling as a whole is highly dependent on serum calcium levels, which, in
turn, are kept in the normal range by a balance between parathyroid hormone, or
PTH, calcitonin and vitamin D.
1. Parathyroid hormone is produced by the parathyroid glands in response to low
serum calcium, and it increases bone resorption to release calcium into the
bloodstream.
2. calcitonin is produced by the thyroid gland in response to high serum calcium, so it
opposes the action of PTH - therefore promoting bone formation and
decreasing bone resorption.
3. vitamin D promotes calcium absorption in the gut, so it increases serum calcium,
promoting bone formation and decreasing bone resorption.
The balance between these regulatory factors results in a peak bone mass, usually by
age 20 to 29 - and this usually occurs earlier in females than in males.
3. strength training increases peak bone mass, as well as hormones
like estrogens and androgens that inhibit bone resorption.
In osteoporosis osteoclasts break down bone faster than the osteoblasts can rebuild, it
results in the lowering of the bone mass and eventually.
These bone changes increase the risk of fracture, and they are known as fragility or
pathologic fractures.
Some bones like the vertebrae, shoulder blades, and ribs consist mainly of spongy
bone, so they are in great risk of fragility fractures.
Factors that accelerate bone mass loss and increase the risk of osteoporosis are :
1. low estrogen levels after menopause
2. low serum calcium.
3. alcohol consumption
4. smoking
5. drugs like glucocorticoids which decrease calcium absorption from the gut through
antagonism of vitamin D
6. drugs like heparin and L-thyroxine.
7. physical inactivity, as seen in astronauts in a zero-gravity environment where they
just don't use their musculoskeletal system as hard as when they’re on earth.As a
result, bone deposition decreases due to a lack of stress, while resorption increases.
8. Turner syndrome, hyperprolactinemia, Klinefelter syndrome, Cushing syndrome,
and diabetes mellitus.
4. the two most common types of osteoporosis are
postmenopausal osteoporosis and senile osteoporosis.
-postmenopausal osteoporosis, decreased estrogen levels lead to increased bone
resorption.
-senile osteoporosis, on the other hand, it’s believed that osteoblasts just gradually lose
the ability to form bone, while the osteoclasts keep doing their thing unabated.bone
resorption usually overtakes bone formation around the 8th decade of life.
People with osteoporosis don’t usually have symptoms until a fracture occurs.
The most common type of fractures are vertebral fractures, also known as compression
fractures, and it occurs when one or more bones in the spine weaken and shatter.
Vertebral fractures cause back pain, height loss, and a hunched posture.
Femoral neck fractures and distal radius fractures can also occur, and they’re often
associated with postmenopausal osteoporosis.
Osteoporosis is usually diagnosed with a dual-energy X-ray absorptiometry or DEXA
scan which tests for bone density.
The test compares an individual's bone density to that of a normal adult which yields the
result or the T score.
A T score less than or equal to -2.5 is diagnostic of osteoporosis.
5. Treatment for osteoporosis
usually relies on bisphosphonate drugs like alendronate and risedronate.
If osteoporosis is really advanced, teriparatide, a recombinant parathyroid hormone can
be used.
Now, even though parathyroid hormone stimulates bone resorption, it’s been found that
intermittent injections with teriparatide activates osteoblasts more than osteoclasts,
therefore increasing bone formation.
Interestingly, a thiazide diuretic like Hydrochlorothiazide can be used to
treat osteoporosis as well.
Hydrochlorothiazide boosts calcium retention in the kidney and directly
stimulates osteoblast differentiation, therefore decreasing mineral bone loss.
Finally, medications like denosumab, which is a monoclonal antibody that
inhibits osteoclasts, and raloxifene, which is a selective estrogen receptor modulator,
can be used for postmenopausal osteoporosis.