Protein-Losing Enteropathy as a Rare Complication of Ketogenic Diet
•
1 recomendación•612 vistas

This case report describes a rare case of a 9-year-old girl who developed protein-losing enteropathy during treatment with the ketogenic diet for intractable epilepsy. The ketogenic diet was started on day 15 of her illness to control seizures. Over time she experienced weight loss and developed hypoproteinemia, hypoalbuminemia, and hypogammaglobulinemia. An albumin scintigraphy revealed tracer accumulation in the small intestine and colon, consistent with protein-losing enteropathy. Her condition improved after discontinuing the ketogenic diet. This represents a rare complication of the ketogenic diet beyond common side effects like hypoproteinemia and its underlying causes require further study.

Recomendados
Más contenido relacionado
La actualidad más candente
La actualidad más candente (20)
Destacado
Similar a Protein-Losing Enteropathy as a Rare Complication of Ketogenic Diet
Similar a Protein-Losing Enteropathy as a Rare Complication of Ketogenic Diet (20)
Más de Takashi Shiihara
Más de Takashi Shiihara (20)
Último
Último (20)
Protein-Losing Enteropathy as a Rare Complication of Ketogenic Diet
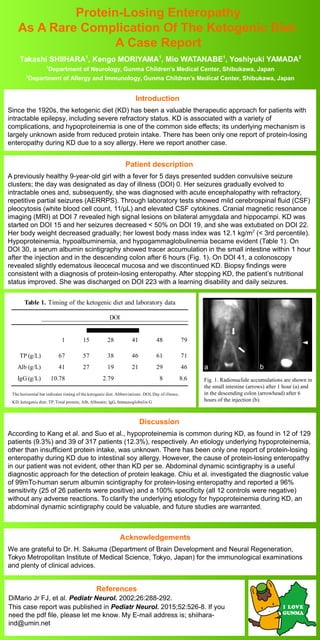
- 1. Protein-Losing Enteropathy As A Rare Complication Of The Ketogenic Diet: A Case Report Introduction Since the 1920s, the ketogenic diet (KD) has been a valuable therapeutic approach for patients with intractable epilepsy, including severe refractory status. KD is associated with a variety of complications, and hypoproteinemia is one of the common side effects; its underlying mechanism is largely unknown aside from reduced protein intake. There has been only one report of protein-losing enteropathy during KD due to a soy allergy. Here we report another case. Takashi SHIIHARA1 , Kengo MORIYAMA1 , Mio WATANABE1 , Yoshiyuki YAMADA2 1 Department of Neurology, Gunma Children’s Medical Center, Shibukawa, Japan 2 Department of Allergy and Immunology, Gunma Children’s Medical Center, Shibukawa, Japan Patient description A previously healthy 9-year-old girl with a fever for 5 days presented sudden convulsive seizure clusters; the day was designated as day of illness (DOI) 0. Her seizures gradually evolved to intractable ones and, subsequently, she was diagnosed with acute encephalopathy with refractory, repetitive partial seizures (AERRPS). Through laboratory tests showed mild cerebrospinal fluid (CSF) pleocytosis (white blood cell count, 11/μL) and elevated CSF cytokines. Cranial magnetic resonance imaging (MRI) at DOI 7 revealed high signal lesions on bilateral amygdala and hippocampi. KD was started on DOI 15 and her seizures decreased < 50% on DOI 19, and she was extubated on DOI 22. Her body weight decreased gradually; her lowest body mass index was 12.1 kg/m2 (< 3rd percentile). Hypoproteinemia, hypoalbuminemia, and hypogammaglobulinemia became evident (Table 1). On DOI 30, a serum albumin scintigraphy showed tracer accumulation in the small intestine within 1 hour after the injection and in the descending colon after 6 hours (Fig. 1). On DOI 41, a colonoscopy revealed slightly edematous ileocecal mucosa and we discontinued KD. Biopsy findings were consistent with a diagnosis of protein-losing enteropathy. After stopping KD, the patient’s nutritional status improved. She was discharged on DOI 223 with a learning disability and daily seizures. Discussion According to Kang et al. and Suo et al., hypoproteinemia is common during KD, as found in 12 of 129 patients (9.3%) and 39 of 317 patients (12.3%), respectively. An etiology underlying hypoproteinemia, other than insufficient protein intake, was unknown. There has been only one report of protein-losing enteropathy during KD due to intestinal soy allergy. However, the cause of protein-losing enteropathy in our patient was not evident, other than KD per se. Abdominal dynamic scintigraphy is a useful diagnostic approach for the detection of protein leakage. Chiu et al. investigated the diagnostic value of 99mTc-human serum albumin scintigraphy for protein-losing enteropathy and reported a 96% sensitivity (25 of 26 patients were positive) and a 100% specificity (all 12 controls were negative) without any adverse reactions. To clarify the underlying etiology for hypoproteinemia during KD, an abdominal dynamic scintigraphy could be valuable, and future studies are warranted. Acknowledgements We are grateful to Dr. H. Sakuma (Department of Brain Development and Neural Regeneration, Tokyo Metropolitan Institute of Medical Science, Tokyo, Japan) for the immunological examinations and plenty of clinical advices. References DiMario Jr FJ, et al. Pediatr Neurol. 2002;26:288-292. This case report was published in Pediatr Neurol. 2015;52:526-8. If you need the pdf file, please let me know. My E-mail address is; shiihara- ind@umin.net DOI 1 15 28 41 48 79 TP (g/L) 67 57 38 46 61 71 Alb (g/L) 41 27 19 21 29 46 IgG (g/L) 10.78 2.79 8 8.6 The horizontal bar indicates timing of the ketogenic diet. Abbreviations: DOI, Day of illness; KD, ketogenic diet; TP, Total protein; Alb, Albumin; IgG, Immunoglobulin G Table 1. Timing of the ketogenic diet and laboratory data Fig. 1. Radionuclide accumulations are shown in the small intestine (arrows) after 1 hour (a) and in the descending colon (arrowhead) after 6 hours of the injection (b).