
Recomendados
Más contenido relacionado
La actualidad más candente
La actualidad más candente (20)
Similar a SURVEY PERFORMA.pdf
Similar a SURVEY PERFORMA.pdf (20)
Más de versha26
Más de versha26 (14)
Último
Último (20)
SURVEY PERFORMA.pdf
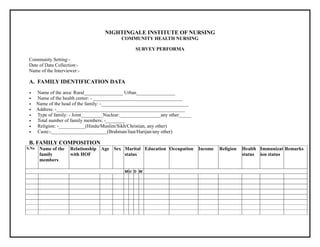
- 1. NIGHTINGALE INSTITUTE OF NURSING COMMUNITY HEALTH NURSING SURVEY PERFORMA Community Setting:- Date of Data Collection:- Name of the Interviewer:- A. FAMILY IDENTIFICATION DATA • Name of the area: Rural________________ Urban________________ • Name of the health center: - _____________________________________ • Name of the head of the family: -____________________________________ • Address: -_____________________________________________________ • Type of family: - Joint_________Nuclear:_________________any other_____ • Total number of family members: -________ • Religion: -___________(Hindu/Muslim/Sikh/Christian, any other) • Caste:-_______________________(Brahman/Jaat/Harijan/any other) B. FAMILY COMPOSITION S.No Name of the family members Relationship with HOF Age Sex Marital status Education Occupation Income Religion Health status Immunizat ion status Remarks M U D W
- 2. C. HOUSEHOLD CHARACTERISTICS 1. General appearance: clean___________dirty_________ 2. Type of house: Pucca______Kuccha_______ (own house/ rented house) 3. Number of rooms: ______________ (adequate/inadequate) 4. Number of person per room: ___ Overcrowding: Present_____Not present 5. Ventilation: Adequate________Inadequate:_____________ (Check for cross ventilation) 6. Electricity: Yes_________ No__________ 7. Source of light: Natural_________ Artificial:________Both:__________ 8. Source of water supply: - Community supply/Household supply/ Tap/Hand Handpump/Well. 9. Place for washing/bathing__________ (separate/ any other (specify) 10. Kitchen facility:-……………separate, Verandha/one corner any other • Cleanliness…………………………clean/Moderately clean / dirty • Chula……………………………. Gas/ electric/ oil mode/ coal /any other 11. Excreta disposal:- Household latrine__________ Community latrine____________Open defcation___________ 12. Spillage water disposal:- Soakage pit________Open drainage_____ Closed drainage_________ 13. Refuse disposal: Dustbin______Fielddisposal_____Burning_____Tipping_____Composting______ 14. Community awareness______________ (yes/no) 14. Sources of environmental pollution_________________ (air/ water/ soil and noise) D. MODE OF TRANSPORT I. Bus service Available/ not available II. Own vehicle If any, specify III. Others E. MEANS OF COMMUNICATION • Radio: yes/ No • TV yes/ No
- 3. • Internet yes/ No • Newspaper yes/ No • Magazine yes/ No • Smart phones yes/No • Landline phones yes/No F. SOCIO-ECONOMIC STATUS 1. Main occupation of the family: ______________________ 2. No. of earning members________________________ 3. Source of the income: ___________________________ Total income of family: __________ Per capita income: ____________ (low/middle/high) 3. PET ANIMALAND POULTRY: _____________ • Pet animal kept in premises__________(yes/no) • Pet animal: Dog/Cow/Goat/Buffalo/any other________________ 4. Habits affecting health: ------tobacco__________- smoking___________-- alcohol________drugs __________ Sedentary life style___________ Note: ___________________ F. NUTRITIONALAND FOOD HYGIENE General nutritional assessment 1. Food preference: vegetarian: ________ non vegetarian:_________egg vegetarian_____ mixed_ 2. Menu for a day: ___________ 3. Staple/ common food of house: ________________ 4. Number of meals per day: _____________________ ANY NUTRITIONAL PROBLEM S.NO. NUTRITIONAL PROBLEM NAME AGE/SEX REMARKS(YES/ NO) 1. Anaemia 2. Malnutrition 3. Goiter 4. Fluorosis
- 4. 5. Worm infection 6. Obesity 7. Vitamin deficiency: if yes specify 8. Food allergy 9. Others G .HEALTH CARE UTILAZATION Practice and availability of health services • Traditional/house remedies:______________ • Goverment hospitals/Health centers:________________ • Privates hospitals/clinics------------------------ • Outlook on causes of disease:- Rational / cures of God / evil spirit/ any other • Outlook of causes of death: Rational/ god wish/ any other • Outlook of prevention of disease: Rational/religions • Awareness of MCH and PHC centre:- Rational / religion • Type of service available:- Satisfied / not satisfied • Have you ever visited the centre:- Yes/No • If yes give reason for visit:- • Any other medical facility:- Yes /No • If yes mention the services • Have you ever availed that services:- Yes/No H. MOTHER AND CHILD HEALTH A. Mother • No. Of pregnancy: ____________ • Type of delivery:_______________(NVD/LSCS/Others) • Place of delivery:_________________(home/institutional) • Prenancy at present__________Yes:____________ No: ________(registered or not) • Regular follow-up______________(yes/no) • If yes, duration of pregnancy: _________________ • Injection TD taken___________(yes/no)
- 5. • Presence of anaemia Yes or no (Hb 8 g or below) Yes:____________No:____________ • Taking treatment (iron/folic acid/calcium) Yes: _________ No:____________(specify if any other)__________ • Any other diseases______________ B. Children (0 to 5 year) • Presence of anaemia Yes:_____________ No:____________ • Under treatment for anaemia; Yes: ___________- No:___________ • Malnutrition: Absent/Mild/Moderate/Severe_____________ • Getting nutritional supplements: Yes:__________ No___________ C Immunization status: S. NO. BCG PENTAVELANT TD OPV MR DPT IPV RVV TYPHOID VITAMIN A BOOSTER ANY OTHER D. FAMILY PLANING 1. No of living children: _______- male_______- female__________ 2. Age of last child ____________Years_________ months__________ 3. Eligible couple for FP ________ Yes___________No__________ 4. Use of family planning methods__________________________ S.NO. F.P. METHODS PRESENTLY USING DISCONTINUED SINCE WHEN REASON FOR DISCONTINUING REMARKS 1 VESECTOMY 2 TUBECTOMY 3 IUD 4 ORAL PILS 5 CONDOM 6 DIAGPHRAM
- 6. 7 JELLY 8 FOAM TAB 9 OTHERS None of the method ever used, reason______________________________________ I. GERIATRIC POPULATION ASSESSMENT Total no of geriatrics: ______________________ 1. Food preference: vegetarian_____________ non vegetarian___________ mixed______________ 2. No. of meal per day: ________________ PERFORMA FOR ELDERLY HEALTH ASSESSMENT; S. NO. HEALTH PROBLEMS 1ST ELDERLY 2ND ELDERLY 3RD ELDERLY 1. Impaired hearing 2. Impaired vision 3. Immobility 4. Incontinence 5. Joint problems 6. Cardio vascular diseases 7. Respiratory diseases 8. DM 9. HTN 10. Neurological diseases 11. Psychological disorders 12. Accident and injuries 13. Dental problems 14. Memory issues 15. Cancers 16. Any other • Financial support during illness:_________________________________________ • Care provider during illness_______________________________________
- 7. • Living with family or not__________________________ J. COMMUNICABLE/NON-COMMUNICABLE DISEASES PREVAILING IN THE FAMILY: S.NO DISEASE NAME AGE/ SEX SIGN& SYMPTOMS DIAGNOSED/UN DIAGNOSED UNDER TREATMENT SINCE WHEN TREATMENT DISCONTINUED SINCE WHEN REMARKS 1 TB 2 LEPROSY 3 MALARIA 4 FILARISIS 5 S.T.D 6 MEASLES 7 CHICKEN POX 8 DM 9 HTN 10 CHD 11 RHD 12 ASTHMA 13 ANY OTHER K. RECORDS OF VITAL EVENTS (BIRTH AND DEATH) In villages reporting of births and deaths are recorded by village Dasis, Chowkidars. When a community health nurse visits the home she comes to know about the birth and deaths taken place since her last visit. The importance of registering these events are: 1. To provide services to new born and mothers to teach her own and child care. 2. To find out the cause of death, necessary and a part of communicable surveillance, particularly in infants, pregnancy and child birth. 3. To teach the community where and why deaths and births to be registered, Births and deaths may be recorded as follows:
- 8. BIRTH RECORDS (WITHIN 1 YEAR) DATE OF BIRTH NAME OF CHILD AGE/SEX NAME AND ADDRESS OF PARENTS NAME OF PERSON ASSISTED IN BIRTH CHILD ALIVE YES/NO WT. AT BIRTH AND PLACE OF DELIVERY. DEATH RECORDS (WITHIN 1 YEAR) S.NO. NAME SEX AGE AT THE TIME OF DEATH PLACE OF DEATH DATE OF DEATH/ CAUSE OF DEATH NAME AND ADDRESS OF PERSON REPORTING DEATH _______________________________________________________________ L. LIST OF NEEDS, PROBLEMS AND NURSING DIAGNOSIS A. NEEDS ………………………………………………………………………………………………………………… ………………………………………………………………………………………………………………… …………………………………………………………………………………………………………………
- 9. ………………………………………………………………………………………………………………… ………………………………………………………………………………………………………………… ………………………………………………………………………………………………………………… ………………………………………………………………………………………………………………… B. PROBLEMS ………………………………………………………………………………………………………………… ………………………………………………………………………………………………………………… ………………………………………………………………………………………………………………… ………………………………………………………………………………………………………………… ………………………………………………………………………………………………………………… ………………………………………………………………………………………………………………… …………………………………………………………………………………………………………………. C. NURSING DIAGNOSIS ………………………………………………………………………………………………………………… ………………………………………………………………………………………………………………… ………………………………………………………………………………………………………………… ………………………………………………………………………………………………………………… ………………………………………………………………………………………………………………… ………………………………………………………………………………………………………………… ………………………………………………………………………………………………………………… ………………………………………………………………………………………………………………… ………………………………………………………………………………………………………………… ………………………………………………………………………………………………………………… ………………………………………………………………………………………………………………… Date of data collection………………………. Signature of supervisor………………