Congenital cyanotic Heart Disease -Dr.Wahid Helmi ., Pediatric consultant . Zarka hospital Demiate
•Descargar como PPT, PDF•
14 recomendaciones•1,066 vistas

Congenital cyanotic Heart Disease

Recomendados
Recomendados
Más contenido relacionado
La actualidad más candente
La actualidad más candente (20)
Similar a Congenital cyanotic Heart Disease -Dr.Wahid Helmi ., Pediatric consultant . Zarka hospital Demiate
Similar a Congenital cyanotic Heart Disease -Dr.Wahid Helmi ., Pediatric consultant . Zarka hospital Demiate (20)
Último
Último (20)
Congenital cyanotic Heart Disease -Dr.Wahid Helmi ., Pediatric consultant . Zarka hospital Demiate
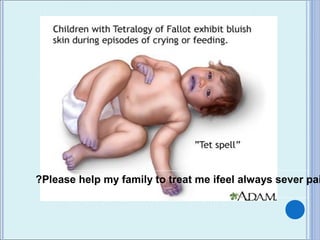
- 1. Please help my family to treat me ifeel always sever pai?
- 2. Congenital Heart Disease Dr.Wahid Helmi ., Pediatric consultant . Zarka hospital Demiate
- 3. Normal Cardiac PressuresNormal Cardiac Pressures 120/<8 25/<5 <5 <8 120/80 25/15
- 4. EchocardiographyEchocardiography Describe the defect . Site of the defect . Location of the defect . Pressure gradient across the defect . Blood flow ,chamre enlargement. Coplications if occured
- 5. Congestive Cardiac FailureCongestive Cardiac Failure Tachycardia Tachypnea Tender enlarged liver Cardiomegaly. FAILURE TO THRIVE Treatment :- ACE-inhibitors - arterial vasodilator / afterload reducing agent Digoxine – increases contractility and decreases heart rate. . Diuretics - enhance renal secretion of sodium and water by reducing circulating blood volume and decreasing preload. Beta Blocker - increases contractility
- 6. Congenital Heart Disease-Congenital Heart Disease- StructuralStructural PINK Shunts ( L to R) : ASD VSD PDA Stenosis: AS PS Coarctation HLHS BLUE TOF TGA Tricuspid atresia Truncus Arteriosus TAPVR Ebstein’s Single ventricle
- 7. Cyanotic Heart LesionsCyanotic Heart Lesions
- 8. CyanosisCyanosis Arterial saturation less than 90% and a PO2 less than 60 torr In all cyanotic heart lesions the amount of cyanosis seen is dependent on the amount of pulm blood flow Decreased PBF- increased cyanosis Increased PBF- minimal cyanosis but CHF may develop With 100% oxygen PO2 <100 is cardiac disease
- 9. 5 “T’s”5 “T’s” Most common cyanotic lesions of the newborn Tetralogy of Fallot Transposition of the Great Arteries Truncus Arteriosus Total Anomalous Venous
- 10. Transposition of the Great ArteriesTransposition of the Great Arteries 5% of all CHD Boys 3:1 Most common cyanotic condition that requires hospitalization in the first two weeks of life
- 11. Transposition of Great Vessels Aorta arises from the right ventricle, and the pulmonary artery arises from the left ventricle - which is not compatible with survival unless there is a large defect present in ventricular or atrial septum. artery aorta
- 12. T G AT G A Aorta arises from the right ventricle & Pulmonary artery arises from the left ventricle → two isolated circulation . After birth there must be amixing defect usually present ( PDA , VSD , ASD) to maintain life . VSD is present in 40% of cases .
- 13. T G AT G A What is the result of separation of the 2 circuits? Hypoxemic blood circulating in the body . Hyperoxemic blood circulating in the pulmonary circuit .
- 15. T G AT G A Defect to permit mixing of 2Defect to permit mixing of 2 circulations :-circulations :- - ASD, VSD, PDA.- ASD, VSD, PDA. VSD is present in 40% ofVSD is present in 40% of casescases Necessary for survivalNecessary for survival..
- 17. Clinical SymptomsClinical Symptoms Depend on anatomy present No mixing lesion and restrictive PFO Profound hypoxia. Rapid deterioration . Death in first hours of life. Absent respiratory symptoms or
- 18. Clinical SymptomsClinical Symptoms Mixing lesion present (VSD or large PDA) Large vigorous infant . Cyanotic . Little to no resp distress. Most likely to develop CHF in first 3-4 months of life, excessive sweating (a cold, clammy
- 19. Chest x-rayChest x-ray Egg-shaped heart in TGA
- 20. ManagementManagement Prostaglandin to establish patency of the ductus arteriosus Increases shunting from aorta into the pulmonary artery Increases pulmonary venous return distending the left atrium Facilitates shunting from the left to the right atrium of fully saturated blood
- 21. ManagementManagement Urgent operation (Rashkind balloon atrial septostomy Procedure) if surgery is not going to be performed immediately. Total correction ( arterial switch ) at 1yea of life .
- 22. Tetralogy of Fallot Four defects are: 1. 2. 3. 4.
- 23. Tetraology of FallotTetraology of Fallot 1. VSD 2. RVOT Obstruction 3. RVH 4. Overriding aorta
- 24. Tetralogy of Fallot (TOF(
- 25. HaemodynamicHaemodynamic When the RV contract in pesence of PS blood is shunted to the overriding aorta leading to central cyanosis . Mild RVD due to pulmonary stenosis . No shunt through the VSD ,
- 26. Clinical Presentation of Cyanotic TOFClinical Presentation of Cyanotic TOF Gradually the mother notice cyanosis (1-2 months), squatting& hypoxic spells. Cyanosis increases with crying & infection . Cyanosis may appear in neonatal period & may be absent (pink fallot) .
- 27. Clinical Presentation of Cyanotic TOFClinical Presentation of Cyanotic TOF Ejection systolic murmur heard at the pulmonary area (from day 1) . During the hyper cyanotic spells the murmur will be very short or inaudible .
- 28. Hypoxic SpellHypoxic Spell (“TET Spell”)(“TET Spell”) Peak incidence of 2-4 months Characterized by: Hyperapnea (Rapid and deep respirations) . Irritability and prolonged crying . Deep attack of cyanosis with crying during fedding .
- 29. Please help my family to treat me ifeel always sever pai?
- 30. Coeur en sabot in tetralogy of Fallot Chest x-rayChest x-ray
- 31. TET Spell TreatmentTET Spell Treatment 1. Hold infant in knee-chest position 2. Sedation &pain relief . 3. Sodium bicarbonate for aidosis . 4. Propranolol (IV):- relief spasm of the infundibulum & causes peripheral vasoconstriction .
- 32. TreatmentTreatment Iron therapy , Palliative shunt operation ( modified Blalock Taussing operation). Total correction at 1 year .
Notas del editor
- Turn into questions
- Case presentation (pink kid turns blue, blue ki)d comes out What would you think about Where does cyanotic heart disease come in? Emailing Dr. Meadows How would you approach this patient? Indications/Contraindications Which kids to start PGE
- Turn into questions
- Make this a question and animate it
- animate
- animate
- animate
- Ask what physiologically happens
- Ask what are the 4 compents and animate