Anatomy of the breast
•Descargar como PPTX, PDF•
267 recomendaciones•77,417 vistas

Anatomy of the breast for medical/dental students. This presentation also contains MCQs to test your knowledge as well as clinical scenario to apply your knowledge.

Recomendados
Más contenido relacionado
La actualidad más candente
La actualidad más candente (20)
Similar a Anatomy of the breast
Similar a Anatomy of the breast (20)
Más de Yapa
Más de Yapa (20)
Último
Último (20)
Anatomy of the breast
- 1. Anatomy of the breast Yapa Wijeratne Faculty of Medicine University of Peradeniya
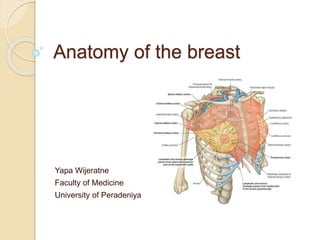
- 3. Modified sweat gland- modified apocrine gland Made up of 15–20 lobules of glandular tissue embedded in fat. Fat accounts for its smooth contour and most of its bulk. These lobules are separated by fibrous septa running from the subcutaneous tissues to the fascia of the chest wall (the ligaments of Cooper/ Astley Cooper fibers/ suspensory ligaments) Between the capsule and the fascia over pectoralis major is the loose connective tissue of the retromammary space.
- 4. Each lobule drains by its lactiferous duct on to the nipple, which is surrounded by the pigmented areola. This area is lubricated by the areolar glands of Montgomery ◦ large, ◦ modified sebaceous glands →may form sebaceous cysts → may infected.
- 6. Naming the quadrants for the purpose of describing a lump Or 1. Upper medial quadrant 2. Upper lateral quadrant 3. Lower medial quadrant 4. Lower lateral quadrant
- 7. Position & extent 2/3 rests on pectoralis major, 1/3 on serratus anterior, while its lower medial edge just overlaps the upper part of the rectus sheath.
- 11. Blood supply
- 12. Axillary artery → ◦ Lateral thoracic (mainly) ◦ Acromiothoracic branches. Internal thoracic (internal mammary) artery → perforating branches; these pierce the 1st – 4th intercostal spaces, then traverse pectoralis major to reach the breast along its medial edge. The 1st & 2nd perforators are the largest of these branches. Intercostal arteries → lateral perforating branches- relatively unimportant source.
- 13. Venous drainage
- 14. Venous drainage Sub areolar venous plexus Posterior intercostal veins communicate with internal vertebral venous plexus veins - therefore cancers can spread to vertebra- may cause back pain
- 17. Follows the pathway of its blood supply along tributaries of the 1. axillary vessels → axillary lymph nodes; 2. internal thoracic vessels → piercing pectoralis major → to traverse each intercostal space → to lymph nodes along the internal mammary chain; these also receive lymphatics penetrating along the lateral perforating branches of the intercostal vessels.
- 18. A subareolar plexus of lymphatics below the nipple (the plexus of Sappey) 75% → axillary 15% → internal mammary Upper → can go to supraclavicular Lower 2 quadrants can go to subdiapragmatic or abdominal nodes
- 21. Development and structure Begins to develop as early as the 4th week as a downgrowth from a thickened mammary ridge (milk line) of ectoderm along a line from the axilla to the inguinal region. Supernumerary nipples or even glands proper may form at lower levels on this line. Lobule formation occurs only in the female breast & does so after puberty. Each lactiferous duct is connected to a tree- like system of ducts and lobules, intermingled & enclosed by connective tissue to form a lobe of the gland.
- 23. The resting (non-lactating) breast, however consists mostly of fibrous & fatty tissue; variations in size are due to variations in fat content, not glandular tissue which is very sparse. During pregnancy alveoli bud off from the smaller ducts & the organ usually enlarges significantly, & more so in preparation for lactation. When lactation ceases there is involution of secretory tissue. After menopause progressive atrophy of lobes & ducts takes place.
- 24. The male breast Resembles the rudimentary female breast has NO lobules or alveoli. The small nipple and areola lie over the 4th intercostal space.
- 26. 1. The retromammary space is located between which of the following structures? (A) skin and the areola (B) pectoralis major and minor (C) breast and deep pectoral fascia (D) suspensory ligament and the skin (E) lactiferous sinus and the nipple
- 27. Answer (C) Between the breast and deep pectoral fascia is a loose connective tissue plane or potential space known as the retromammary space
- 28. 2.The mammary glands are modified versions of which type of gland? (A) sebaceous gland (B) lymph gland (C) sweat gland (D) tonsillar tissue (E) endocrine gland
- 29. Answer (C) The mammary glands are modified sweat glands
- 30. 3. Which of the following does NOT supply the breast with blood? (A) lateral thoracic artery (B) thoracoacromial artery (C) posterior intercostals arteries (D) internal thoracic artery (E) costoclavicular artery
- 31. Answer (E) The breast is supplied by the 1. internal thoracic, 2. lateral thoracic, 3. thoracoacromial, and posterior 4. intercostal arteries
- 32. 4. The high death rate associated with breast cancer is related to which of the following? (A) nerve supply (B) blood supply (C) venous drainage (D) poor imaging techniques (E) complex lymphatic drainage
- 33. Answer (E) Because the axillary lymph nodes are the most common site of metastases from a breast cancer, enlargement of the palpable nodes in a woman suggests the possibility of breast cancer and may be key to early detection. However, the absence of enlarged axillary nodes is no guarantee that metastasis from a breast cancer has not occurred, because the malignant cells may have passed to other nodes, such as the infraclavicular and supraclavicular lymph nodes
- 34. 5. Which statement most appropriately describes the female breast? 1. It overlies the 3rd to 8th ribs. 2. It consists of 2–3 lobules. 3. It has suspensory ligaments, which tether the dermis to the fascia of the chest wall. 4. The retro-mammary space lies deep to pectoralis major. 5. The areolar glands are responsible for lactation.
- 35. Answer c. The dermis is tethered to the breast ducts and the deep fascia overlying pectoralis major by fibrous strands known as the suspensory ligaments of Cooper. As these atrophy and weaken with age the breast becomes more pendulous.
- 36. Explanations a. The base of the adult female breast consistently overlies the 2nd to 6th ribs, from the sternal edge to the midaxillary line. The upper outer quadrant extends towards the axilla as the “axillary tail”. b. The breast consists of 15–20 lobules of glandular tissue, all individually drained by a corresponding lactiferous duct, which empty at the nipple via the lactiferous sinus. d. The retro-mammary space is located between the posterior capsule of the breast and the fascia over pectoralis major. This space is commonly exploited in the placement of implants. e. The areolar glands of Montgomery are modified sebaceous glands located beneath the areola and are responsible for lubricating the area. These glands may enlarge or become infected, especially during pregnancy.
- 37. 6. Which of these statements are true considering the vasculature and lymphatic drainage of the breast? 1. The main blood supply is derived from branches of the internal mammary artery. 2. Venous drainage is predominantly to the internal mammary vein. 3. Lymphatic drainage is divided evenly between the axillary and internal mammary nodes. 4. The superficial lymphatics of each breast remain separate in healthy people. 5. All the axillary lymphatics drain through the apical axillary nodes.
- 38. Answer e. There are five main groups of nodes in the axilla. The anterior, posterior, lateral and central groups empty into the apical group. The apical nodes drain into the subclavian lymph trunk.
- 39. Explanations a. The main supply is via the lateral thoracic and thoracoacromial branches of the axillary artery. The internal mammary (internal thoracic) artery supplies a significant part of the medial aspect via perforating branches. The posterior intercostal arteries also make a minor contribution. b. Venous drainage follows the arterial supply of the breast and is primarily to the axillary vein. c. Approximately 75% of drainage is to the axillary lymph nodes, primarily to the anterior group. The majority of the remaining drainage, especially of the medial part, is to the internal mammary nodes. d. The superficial lymphatics have connections with the opposite breast and anterior abdominal wall. If the normal drainage channels become obstructed by malignant disease, metastatic spread may, therefore, occur to the contralateral breast or axillary nodes.
- 40. Name the anatomical structure/s involved Pt who is found to have a breast lump also having a lump in the axilla? LN enlargement There is a dimpling of the overlying skin of the breast Suspensory ligaments of Cooper- lump is pulling down the fibers. You suspect it is malignant & try to move the lump while the pt presses her hip with her hands. Lump movement reduces. Involvement of the pectoralis major & fascia
- 41. What directions would you move the lump? Diagonally to the midline
- 42. Pt is now undergoing a mastectomy. Surgeon found LN involvement. He wants to assess the level of involvement. What is the landmark would you choose? Pectoralis minor
- 43. If she is willing to reconstruct the breast, what muscles can be used? Latissimus dorsi muscle (an LD flap) Transversus abdominis muscle (TRAM flap)
- 44. Now the Pt has undergone the L/S mastectomy. She complains of L/S upper limb swelling. Removal of axillary LNs which drains L/s upper limb lymphatics Pt also complains of parasthesia of the left axillae Damage to the left intercostobrachial nerve
- 45. Thank you!