Nephrotic vs nephritic syndrome
•
142 recomendaciones•74,652 vistas

A comparison between Nephritic and Nephrotic syndrome from Professor Hossam Mowafy Internal Medicine textbook nephrology section, Please inform me if there is any error or wrong information include.

Recomendados
Más contenido relacionado
La actualidad más candente
La actualidad más candente (20)
Similar a Nephrotic vs nephritic syndrome
Similar a Nephrotic vs nephritic syndrome (20)
Más de Hatem Refaat El-Sheemy
Más de Hatem Refaat El-Sheemy (11)
Último
Último (20)
Nephrotic vs nephritic syndrome
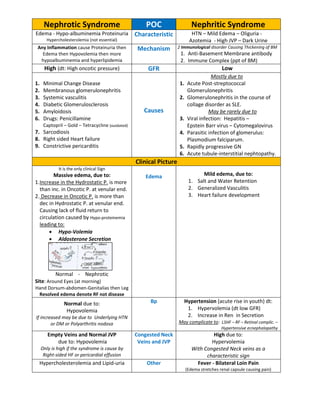
- 1. Nephrotic Syndrome POC Nephritic Syndrome Edema - Hypo-albuminemia Proteinuria Hypercholesterolemia (not essential) Characteristic HTN – Mild Edema – Oliguria - Azotemia - High JVP – Dark Urine Any Inflammation cause Proteinuria then Edema then Hypovolemia then more hypoalbuminemia and hyperlipidemia Mechanism 2 Immunological disorder Causing Thickening of BM 1. Anti-Basement Membrane antibody 2. Immune Complex (ppt of BM) High (dt: High oncotic pressure) GFR Low 1. Minimal Change Disease 2. Membranous glomerulonephritis 3. Systemic vasculitis 4. Diabetic Glomerulosclerosis 5. Amyloidosis 6. Drugs: Penicillamine Captopril – Gold – Tetracycline (outdated) 7. Sarcodiosis 8. Right sided Heart failure 9. Constrictive pericarditis Causes Mostly due to 1. Acute Post-streptococcal Glomerulonephritis 2. Glomerulonephritis in the course of collage disorder as SLE. May be rarely due to 3. Viral infection: Hepatitis – Epstein Barr virus – Cytomegalovirus 4. Parasitic infection of glomerulus: Plasmodium falciparum. 5. Rapidly progressive GN 6. Acute tubule-interstitial nephtopathy. Clinical Picture It is the only clinical Sign Massive edema, due to: 1.Increase in the Hydrostatic P. is more than inc. in Oncotic P. at venular end. 2. Decrease in Oncotic P. is more than dec in Hydrostatic P. at venular end. Causing lack of fluid return to circulation caused by Hypo-proteinemia leading to: Hypo-Volemia Aldosterone Secretion Normal - Nephrotic Site: Around Eyes (at morning) Hand Dorsum-abdomen-Genitalias then Leg Resolved edema denote RF not disease Edema Mild edema, due to: 1. Salt and Water Retention 2. Generalized Vasculitis 3. Heart failure development Normal due to: Hypovolemia If increased may be due to Underlying HTN or DM or Polyarthritis nodosa Bp Hypertension (acute rise in youth) dt: 1. Hypervolemia (dt low GFR) 2. Increase in Ren in Secretion May complicate to: LSHF – RF – Retinal complic. – Hypertensive ecnephalopathy Empty Veins and Normal JVP due to: Hypovolemia Only is high if the syndrome is cause by Right-sided HF or pericardial effusion Congested Neck Veins and JVP High due to: Hypervolemia With Congested Neck veins as a characteristic sign Hypercholesterolemia and Lipid-uria Other Fever - Bilateral Loin Pain (Edema stretches renal capsule causing pain)
- 2. Nephrotic Syndrome POC Nephritic Syndrome Mainly Lab. Clinical: by exclusion Urine Analysis Usually Normal Volume Low (but above 400cc/day) Above 3-3.5gm/day (S or NS, S is better) Proteinuria Very low Normal (slight elevation dt amino acids) Specific Gravity High (as tubules are normal) Maybe indicating GN as a cause With Hyaline Cast and THP RBCs and RC Present: a Sure Diagnostic Sign (Tamm–Horsfall Protein) Mostly Normal To assess renal function Urea/Creatinine Elevated in severe cases Blood LOW Serum Protein Usually Normal Normal Sodium Possibly Increase Decreased Potassium Possibly Increase Early: normal Later: High dt RF Urea/Creatinine Possibly Increase High Cholesterol (but not essential) Low Calcium (but not ionized Ca = no tetany) Other: Biopsy: Crescent form Treatment Water: given with negative balance. High Protein – High Calcium Salt Restriction Potassium: given freely Diet Water: Restricted with negative balance Less than normal (as pt. is hypervolemic) Sodium and Potassium restriction Protein Restriction Look for the underlying cause Diuretics: Spironolactone - mannitol Albumin infusion – Calcium Antibiotics: as pt is immunocomp. Empirical Steroids: is the pt is responding? Drugs Immuno-Suppressor: non-steroidal Anti-Hypertensive: Best is alpha-methyl dopa (inc Renal B-flow too) and avoid ACE Diuretics: avoid cortico-medullary in balance Antibiotics Dialysis If Renal Failure occured Source: Professor Dr.Hossam Mowafy Textbook and Lecture S By: Hatem Refaat El-Sheemy Undergraduate MBBCH – MUST – College of Medicine