11. ACHALASIA
• “Failure to relax”
– Aperistalsis
– Incomplete relaxation of the LES
– Increased LES tone
• INCREASE: Gastrin, serotonin, acetylcholine,
Prostaglandin F2α, motulin, Substance P, histamine,
pancreatic polypeptide
• DECREASE: N.O., VIP
– Progressive dysphagia starting in teens
– Mostly UNCERTAIN etiology
12. HIATAL HERNIA
• Diaphragmatic muscular defect
• WIDENING of the space which the lower
esophagus passes through
• IN ALL cases, STOMACH above
diaphragm
• Usually associated with reflux
• Very common Increases with age
• Ulceration, bleeding, perforation,
strangulation
19. VARICES
• THREE common areas of portal/caval anastomoses
–Esophageal
– Umbilical
– Hemorrhoidal
• 100% related to portal hypertension
• Found in 90% of cirrhotics
• MASSIVE, SUDDEN, FATAL hemorrhage is the most
feared consequence
26. BARRETT’S
ESOPHAGUS
• Can be defined as intestinal metaplasia of a normally
SQUAMOUS esophageal mucosa. The presence of
GOBLET CELLS in the esophageal mucosa is
DIAGNOSTIC.
• SINGLE most common RISK FACTOR for esophageal
adenocarcinoma
• 10% of GERD patients get it
• “BREACHED” G-E junction
29. BARRETT’S
ESOPHAGUS
• INTESTINALIZED (GASTRICIZED) mucosa is AT RISK
for glandular dysplasia.
• Searching for dysplasia when BARRETT’s is present
is of utmost importance
• MOST/ALL adenocarcinomas arising in the
esophagus arise from previously existing
BARRETT’s
30.
31. ESOPHAGITIS
• CHEMICAL
– LYE (suicide attempts) with strictures
– Alcohol
– Extremely HOT drinks
– CHEMO (often harmful to ALL high turnover
mucosas)
• INFECTIOUS
– HSV, CMV, Fungal (especially CANDIDA)
45. ANATOMY Body (acid),
Cardia (esoph), Fundus (diaph),
Antrum, Pylorus
Greater/Lesser Curvatures
1500-3000 ml
Rugae
INNERVATION: VAGUS, Sympathetic
VEINS: Portal
Blood Supply: RG, LG, RGE(O), LGE(O), SG, ALL 3
branches of the celiac, no matter what the
variations may be.
46.
47.
48.
49.
50.
51. CELLS
MUCOUS: MUCUS, PEPSINOGEN II
CHIEF: PEPSINOGEN I, II
PARIETAL: ACID
ENTEROENDOCRINE: HISTAMINE,
SOMATOSTATIN, ENDOTHELIN
59. GASTRITIS
• CHRONIC, NO EROSIONS, NO HEMORRHAGE
•
Chronic infection by
H. pylori
• Immunologic (autoimmune), e.g., PA
• Toxic, as with alcohol and cigarette smoking
• Postsurgical, reflux of bile
• Motor and mechanical, including obstruction, bezoars (luminal
concretions), and gastric atony
• Radiation
• Granulomatous conditions (e.g., Crohn disease)
• GVH, uremia
60. GASTRITIS
• CHRONIC, NO EROSIONS, NO HEMORRHAGE
• Perhaps some neutrophils
• Lymphocytes, lymphoid follicles
• REGENERATIVE CHANGES
– METAPLASIA, intestinal
– ATROPHY, mucosal hypoplasia, “thinning”
– DYS-PLASIA
63. GASTRITIS
• OTHER
– EOSINOPHILIC, middle aged women
– ALLERGIC, children (also eosinophils)
– LYMPHOCYTIC, T-Cells, body, DIFFUSE
– GRANULOMATOUS, Crohn’s, other granulomas
– GVH, in bone marrow transplants
64.
65. •
•
•
•
•
•
“PEPTIC” ULCERS
“PEPTIC” implies acid cause/aggravation
ULCER vs. EROSION (muscularis mucosa intact)
MUCSUBMUCMUSCULARISSEROSA
Chronic, solitary (usually), adults
80% caused by H. pylori
100% caused by H. pylori in
duodenum
• NSAIDS
“STRESS”
67. •
•
•
•
“PEPTIC” ULCERS
Gnawing, burning, aching pain, epigastric
Fe deficiency anemia
Acute hemorrhage
Penetration, perforation:
– Pain in BACK
– Pain in CHEST
– Pain in LUQ
• NOT felt to develop into malignancy
68. • Bleeding
“PEPTIC” ULCERS
– Occurs in 15% to 20% of patients
– Most frequent complication
– May be life-threatening
– Accounts for 25% of ulcer deaths
– May be the first indication of an ulcer
• Perforation
– Occurs in about 5% of patients
– Accounts for two thirds of ulcer deaths
– Rarely, is the first indication of an ulcer
• Obstruction from edema or scarring
– Occurs in about 2% of patients
– Most often due to pyloric channel ulcers
– May also occur with duodenal ulcers
– Causes incapacitating, crampy abdominal pain
– Rarely, may lead to total obstruction with intractable vomiting
75. “HYPERTROPHIC” GASTROPATHY
• Inaccurate name “hypertrophic gastritis”
• Ménétrier disease, resulting from profound hyperplasia
of the surface mucous cells with accompanying
glandular atrophy, ass. w. CMV, H. Pylori, ↑TGF-α
• Hypertrophic-hypersecretory gastropathy, associated
with hyperplasia of the parietal and chief cells within
gastric glands (normal gastrin)
• Gastric gland hyperplasia secondary to excessive
gastrin secretion, in the setting of a gastrinoma
(Zollinger-Ellison syndrome)
76.
77. GASTRIC “VARICES”
• SAME SETTING AND ETIOLOGY AS
ESOPHAGEAL VARICES, i.e., PORTAL
HYPERTENSION
• NOT AS COMMON AS ESOPHAGEAL VARICES
• MAY LOOK LIKE PROMINENT RUGAE
• IF A PATIENT HAS GASTRIC VARICES, HE ALSO
PROBABLY HAS ESOPHAGEAL, (but probably
not vice versa)
78. GASTRIC TUMORS
• BENIGN:
*
– “POLYPS ” (HYPERPLASTIC vs. ADENOMATOUS)
– LEIOMYOMAS (Same gross and micro as smooth muscle)
– LIPOMAS (Same gross and micro as adipose tissue)
• MALIGNANT
– (ADENO)-Carcinoma
– LYMPHOMA
• POTENTIALLY MALIGNANT
– G.I.S.T. (Gastro-Intestinal “Stromal” Tumor)
– CARCINOID (NEUROENDOCRINE)
91. G.I.S.T. TUMORS
• Can behave and/or look benign or
malignant
• Usually look like smooth muscle, i.e.,
“stroma”, “spindly”
• Are usually POSITIVE for
c-KIT (CD117), i.e.,
express this antigen on
immunochemical staining, the tumor
cells are derived from the interstitial
cells of Cajal, a “neural” type of cell,
similar to the neural plexi found in the
intestines.
109. VIRAL enterocolitis
• Rotavirus most common, by far
– Selectively infects and destroys
mature enterocytes in the small
intestine
– Crypts spared
• Most have a 3-5 day course
• Person to person, food, water
110. BACTERIAL enterocolitis
• Ingestion of bacterial toxins
– Staph
– Vibrio
– Clostridium
• Ingestion of bacteria which produce toxins
– Montezuma’s revenge (traveller’s diarrhea), E.coli
• Infection by enteroinvasive bacteria
– Enteroinvasive E. coli (EIEC)
– Shigella
– Clostridium difficile
111. E. coli
•
•
•
•
Toxin, invasion, many subtypes
Food, water, person-to-person
Usually watery, some hemorrhagic
INFANTS often, in epidemics
117. BACTERIAL OVERGROWTH
SYNDROME
• One of the main reasons why “normal” gut
flora is NOT usually pathogenic, is because,
they are constantly cleared by a NORMAL
transit time.
•
•
•
•
BLIND LOOPS
DIVERTICULA
OBSTRUCTION
Bowel PARALYSIS
126. CELIAC DISEASE
• Also called SPRUE
• Also called NON-tropical SPRUE
• Also called GLUTEN-SENSITIVE ENTEROPATHY
– Sensitivity to GLUTEN, a wheat protein, gliadin
– Immobilizes T-cells
– Also in oat, barley, rye
– Progressive mucosal “atrophy”, i.e. villous flattening
– Relieved by gluten withdrawal
134. (I) IBD
• COMMON FEATURES
–IDIOPATHIC
–DEVELOPED COUNTRIES
–COLONIC INFLAMMATION
–SIMILAR Rx
–BOTH have increased CANCER RISK
135. (I) IBD DIFFERENCES
• CROHN (CD)
• ULCERATIVE (UC)
– TRANSMURAL, THICK WALL
– MUCOSAL, THICK MUCOSA
– NOT LIMITED to COLON
– LIMITED to COLON
– GRANULOMAS
– NO GRANULOMAS
– FISTULAE COMMON
– FISTULAE RARE
– TERMINAL ILEUM OFTEN
– TERMINAL ILEUM NEVER
– SKIP AREAS
– NO SKIP AREAS
– “CRYPT” ABSCESSES NOT COMMON
– “CRYPT” ABSCESSES COMMON
– NO PSEUDOPOLYPS
– PSEUDOPOLYPS
– MALABSORPTION
– NO MALABSORPTION
145. Formation of colonic diverticuli
• The most commonly known colonic diverticuli are pseudo
diverticuli – composed of only mucosa on the luminal side and
serosa externally. Why are these called “pseudo” or false?
• Diverticuli resemble hernias of the colonic wall in that they occur @
sites of entry of mucosal arteries as they pass through the
muscularis – this represents a weak spot that leads to a
diverticulum if the individual generates high colonic intraluminal
pressure (low fiber diet)
154. POLYPS
• ANY mucosal bulging, blebbing, or bump
• HYPERPLASTIC
(NON-NEOPLASTIC)
• HAMARTOMATOUS (NON-NEOPLASTIC)
• ADENOMATOUS
(TRUE NEOPLASM, and
regarded by many as “potentially” PRE-MALIGNANT as well)
• SESSILE vs. PEDUNCULATED
• TUBULAR vs. VILLOUS
172. Tumor Stage
Histologic Features of the Neoplasm
Tis
Carcinoma in situ (high-grade dysplasia) or intramucosal
carcinoma (lamina propria invasion)
T1
Tumor breaches the musc. muc. invades into submucosa
T2
Extending into the muscularis propria but not penetrating
through it
T3
Penetrating through the muscularis propria into subserosa
T4
Tumor directly invades other organs or structures
Nx
Regional lymph nodes cannot be assessed
N0
No regional lymph node metastasis
N1
Metastasis in 1 to 3 lymph nodes
N2
Metastasis in 4 or more lymph nodes
Mx
Distant metastasis cannot be assessed
M0
No distant metastasis
M1
Distant metastasis
173. OTHER TUMORS
• CARCINOID, with or without
syndrome
• LYMPHOMA (MALTOMAS, B-Cell)
• LEIOMYOMA/-SARCOMA
• LIPOMA/-SARCOMA
174. ANAL CANAL CARCINOMAS
• MORE LIKELY TO BE SQUAMOUS, or
“basaloid”
• WORSE IN PROGNOSIS
• HPV RELATED
176. ANATOMY
• Junction of 3 tenia coli, variable in location
• All 4 layers, true serosa
• Thickest layer is submucosal lymphoid tissue
•
•
•
•
APPENDICITIS (ACUTE)
MUCOCELE
MUCUS CYSTADENOMA
MUCUS CYSTADENOCARCINOMA
177. ACUTE APPENDICITIS
• GENERALLY, a disease of YOUNGER people
• OBSTRUCTION by FECALITH the classic cause but
fecaliths present only about half the time
• EARLY APPENDICITIS: NEUTROPHILSMucosa,
submucosa
• NEED NEUTROPHILS in the MUSCULARIS
to confirm the DIAGNOSIS
• 25% normal rate, usually
• Perforationperitonitis the rule, if no surgery
184. PERITONEUM
• Visceral, Parietal: all lined by mesothelium
• Peritonitis, acute:
– Appendicitis, local or with rupture
– Peptic ulcer, local or ruptured
– Cholecystitis, local or ruptured
– Diverticulitis, local or with rupture
– Salpingitis gonococcal or chlamydial,
retrograde or perforated
– Ruptured bowel due to any reason
– Perforating abdominal wall injuries
188. TUMORS
• MESOTHELIOMAS (solitary nodules or
diffuse constricting growth pattern, also
asbestos caused)
• METASTATIC, usually diffuse, often
looking very much like pseudomyxoma
peritoneii, but containing tumor cells,
usually adenocarcinoma
Notas del editor
*Serosa when it becomes intra-abdominal.
Let’s “shotgun” this esophagus! You know the drill 1,2,3,4
DYSPHAGIA = difficulty swallowing, a non-specific, generic term.
ACHALASIA, (pronounced /e-kə-lesia) also known as esophageal achalasia, esophagospasm, achalasia cardiae, cardiospasm, and esophageal aperistalsis, is an esophageal motility disorder involving the smooth layer of the esophagus and the lower esophageal sphincter (LES). It is characterized by incomplete LES relaxation, increased LES tone, and aperistalsis of the esophagus (inability of smooth muscle to move food down the esophagus) in the absence of other explanations like cancer or fibrosis. Achalasia is characterized by difficulty swallowing, regurgitation, and sometimes chest pain.
Common motility disorders. Note that the classical ZENKER diverticulum is usually in the UPPER esophagus and pouches posteriorly.
Generally synonymous with the word “esophagospasm”
Of the three major tubes that traverse the diaphragm, the esophagus has the weakest surroundings, much more muscular and less fibrous than the aorta and IVC.
HH can be thought of as a sequela of chronic gastric overdistention.
Hiatal hernia with SHATZKI ring.
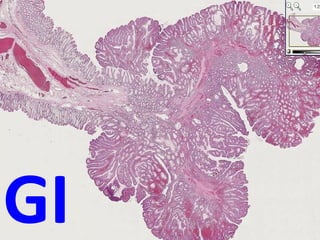
“TRUE” diverticula usually have all 4 layers in its wall: Muc/Submuc/Musc/Adventitia. Which one of these might be the most closest linked with dysphagia? Ans: Zenkers
Note that the image on the right is the NON-microscopic demonstration of a squamo-columnar junction.
Any chronically increased venous pressure phenomenon which dilates a vein, will also make it more tortuous---legs or esophagus!
Endoscopist’s point of view (left), and one of the treatment options (right). “Banding”, i.e., putting rubber bands on the varices, is also common.
GERD is as MASSIVELY common as heartburn itself, because it IS heartburn!!!
If we said that chronic gastric over distension was the usual cause of hiatal hernia, we can also say this for GERD as well.
Do mucous cells secrete a mild alkaline protective pH? Answer: YES
You can think of Barrett’s as REVERSE squamous metaplasia.
You should have, by now, a good feel for squamous (shiny) vs. columnar (mucoid) surface mucosas anywhere in the body.
Barrett’s on top, goblet cell on right, normal esophagus on bottom.
Glandular “dysplasia”. Find the atypical cells.
Candida, candida esophagitis in a HIV positive patient often is indicative of “full blown” AIDS.
Herpes, from the points of view of the endoscopist and the pathologist. Might these large nucleolated cells be exfoliated as “Tzanck” cells? Answer: YES
The very BEST way to classify ALL tumors of a major organ is to remember its basic HISTOLOGY.
You do NOT need to memorize a stupid list from a pathology lecture, just remember an organ’s native cells!
Would you call this squamous “dysplasia”? Answer: YES
Would your fear it would develop into squamous cell carcinoma? Answer: YES
Does it always? Answer: NO
Does it usually? Answer: With time, YES, but that time may be years and years.
Why is a cancer in the LOWER part of an esophagus MUCH less likely to be SQUAMOUS, than in the UPPER part? Answer: Barretts.
Is Barrett’s, by itself, PRE-malignant? Answer: NO!!!
The transition of a normally squamous esophageal mucosa to a glandular or “intestinal” type of a mucosa is called BARRETTS.
Moving down the GI tract, next stop: Stomach!
ALL 3 classic branches of the celiac axis supply the stomach: Common hepatic, left gastric, and splenic
If you think of the acid production in the stomach to be ONLY in the mid-BODY, and the proximal and distal ends as chiefly mucous to protect the esophagus and duodenum from the harsh acid, then you will understand the histology.
GE Junction is a squamo-columnar junction. Do you see a distinct LGE “sphincter”? Answer: NO
Remember that BOTH the proximal and distal ends of the stomach NEUTRALIZE acid with alkaline MUCUS, rather than PRODUCE acid.
Body with numerous chief and parietal (acid producing) cells.
Pyloric sphincter, note a few submucosal glands seen a little BEFORE the sphincter itself.
Somatostatin (also known as growth hormone-inhibiting hormone (GHIH) or somatotropin release-inhibiting factor (SRIF)) is a polypeptide that regulates the endocrine system and affects neurotransmission and cell proliferation via interaction with G-protein coupled somatostatin receptors and inhibition of the release of numerous secondary hormones.
Endothelins are proteins that constrict blood vessels and raise blood pressure.
Pepsinogens are PRECURSORS of protein hydrolyzing pepsins, having a few (~44) more polypeptides.
• The cephalic phase, initiated by the sight, taste, smell, chewing, and swallowing of palatable food, is
mediated by vagal activity.
• The gastric phase involves stimulation of stretch receptors by gastric distention and is mediated by vagal impulses; it also involves gastrin release from endocrine cells, the G cells, in the antral glands. Gastrin release is promoted by luminal amino acids and peptides and possibly by vagal stimulation.
• The intestinal phase, initiated when food containing digested protein enters the proximal small intestine, involves a number of polypeptides besides gastrin.
Prostaglandin E both DECREASES acid and INCREASES mucous.
Remember the stomach develops, like the lungs, from the FOREGUT, if you want to understand developmental anomalies.
What do you think the baby’s #1 symptom would have to be? Answer: VOMITING
The acute/chronic patterns of gastritis generally conform to the poly/mono principles we so often have referred to. The “other” category of gastritis are also histologically based.
The concepts and histologic changes in acute and chronic follow of course the classic histologic principles:
Acute polys
Chronic monos
However, the main CLINICAL differentiation between acute and chronic gastritis would be the presence or absence of blood, respectively.
The concepts and histologic changes in acute and chronic follow the classic histologic principles:
Acute polys
Chronic monos
ACUTE gastritis Hemorrhage, “erosions”, neutrophils (i.e., “POLYS”)
CHRONIC gastritis MONOS, NO hemorrhage, NO erosions
And do not forget: CHRONIC of the follows ACUTE
Helicobacter pylori, gastric biopsy, silver stain on left, Giemsa stain on right. As a rule, these bugs ADHERE closely to the gastric mucin rather than invade the epithelial cells.
Would an autoimmune gastritis be associated with megaloblastic anemia? Why? Answer: DECREASED intrinsic factor
No doubt achlorhydria is the common factor of chronic gastritis and B12 megaloblastic anemias
Eosinophilic gastritis.
If these were granulomas rather than eosinophils, what kind of gastritis would it be? (rhetorical question)
Would this slide be seen in a REAL classroom to those sitting in the back row?
Please remember acute “stress” ulcers are highly related to an EXCESS of endogenous or exogenous steroids.
Not surprisingly, acute “ulcers” are likened to acute “gastritis”. Does this list look familiar?
This type of acute “stress” ulcer is often confused with ulceration from gastric intubation, but intubation ulcers are usually more linear and less diffuse.
It is not at all unusual to see, at autopsy, stomachs that look like this in people whose death was preceded by extreme physiologic stress.
No doubt you will attend surgical grand rounds on bezoars from time to time.
A large obstructive bezoar usually takes on the shape and contour of the stomach
*Probably better termed “hyperplastic” by the traditional classical definition, but, conventionally, called “hypertrophic”.
Note that the “hypertrophy” is really various types of “hyperplasia”.
Note prominence or “cerebrated” appearance of rugae.
Hyperplastic gastric mucosa necessitates an increase in surface area, i.e., rugal prominence.
In general. A “polyp*” can be thought of as ANYTHING which projects as a bump or nodule from a mucosal surface.
HYPERPLASTIC POLYPS are considered to be NON-neoplastic, and therefore NEVER turn into cancers. ADENOMATOUS polyps are true benign neoplasms and MAY turn into carcinomas, particularly if the exhibit DYSPLASIA on biopsy.
This SAME general principle, is even MORE true of the colon!
But in general, you know the drill: 1) Benign, 2) Malignant, and 1) epithelial, 2) stromal, and 3) lymphoid
The concept of GASTRIC polyps generally follows the concepts of COLONIC polyps, i.e., HYPERPLASTIC are ALL benign with many different types of cells, and ADENOMATOUS are more “associated” with malignancy, but are NOT NECESSARILLY pre-malignant.
* WHY? ANS: Poorer people eat more nitrated preserved foods? Spicy foods? Less fresh foods?
These are logical anatomic or “geometric” descriptions, and NOT exact classifications.
The LINITIS PLASTICA is the most SPECTACULAR, and most FEARED, of all gastric adenocarcinomas. It grows DIFFUSELY through all layers of the stomach, greatly thickening its wall, and giving the stomach a classic LEATHER BOTTLE appearance. It has a horrible prognosis.
DIFFUSE WALL THICKENING of ALL FOUR STOMACH LAYERS IS THE RULE!!!!!!!
NOT ONLY DOES IT BEHAVE LIKE WILDFIRE BUT IS ALSO POORLY DIFFERENTIATED “SIGNET” CELLS, DIFFUSELY INFILTRATIVE.
Classical papilla! Malignant too.
Of course, you would NEVER call this squamous.
If you thought this yucky whitish stuff was mucin, what stain would you order to prove it? Answer: Mucicarmine stain.
Is a positive muci-CARMINE stain RED (i.e., “carmine” colored)? Answer: YES
Signet ring cells are POORLY differentiated adenocarcinoma cells, and are OFTEN seen with linitis plastica. Could those large “holes” in the cytoplasm possibly be mucicarmine positive” Answer: YES
How can you have a squamous cell carcinoma of the stomach if the stomach has no normal squamous cells normally? Ans: SQUAMOUS METAPLASIA. The squamous component is usually NOT malignant
For as notoriously complex as all this sounds, they look like boring leiomyomas, and in the days PRE-immunochemistry, they probably WERE inaccurately called smooth muscle tumors, i.e., leiomyomas.
Most of the pathology concepts are logical and easy. A couple are a little involved.
How does about 5 square feet turn into a tennis court?
Why is the middle and inferior rectal artery so different from the superior? ANS: They do NOT come from the IMA
The SI has a “villous” or “papillary”, i.e., hairy surface appearance, while the LI has a configuration similar to the stomach, i.e., “pits and glands”
MALT lymphoid tissue (redundant) is rich in th lamina propria of the mucosa and extends throughout the submucosa too. Why? Answer: To secrete IgA and other antibodies against potential pathogens.
Please review these hormones to understand their function:
Approximately 80 percent of the human body's total serotonin is located in the enterochromaffin cells in the gut, where it is used to regulate intestinal movements.
Somatostatin is classified as an inhibitory hormone to growth hormone, appropriately named, of course.
Motilin is secreted by endocrine M cells (these are not the same M cells that are in Peyer's patches) that are numerous in crypts of the small intestine. Motilin stimulates peristalsis.
Cholecystokinin a peptide hormone of responsible for stimulating the digestion of fat and protein and is synthesized by I-cells in the mucosal epithelium of the small intestine to stimulate the pancreas and gallbladder to release enzymes.
Gastric inhibitory polypeptide (GIP), also known as the glucose-dependent insulinotropic peptide is a member of the secretin family of hormones. It induces insulin secretion, and is primarily secreted by the duodenum..
Neurotensin is a 13 amino acid neuropeptide that is implicated in the regulation of LH and prolactin release and has significant interaction with the dopamine system.
VIP seems to induce GI smooth muscle relaxation.
Enteroglucagon is a peptide hormone secreted from mucosal cells primarily of the colon and terminal ileum. It has 37 amino acids. Enteroglucagon is released following ingestion of a mixed meal, and delays gastric emptying.
What is the difference between Peyer patches and MALT? Answer: Peyer patches are MALT of the Ileum. Originally they were described in the distal ileum.
Gastroschisis is also called paraomphalocele, laparoschisis, or abdominoschisis. Gastroschisis is a birth defect in which an infant's intestines stick out of the body through a defect on one side of the umbilical cord.
Similarly, omphalocoele is a type of abdominal wall defect in which the intestines, liver, and occasionally other organs remain outside of the abdomen in a sac because of a defect in the development of the muscles of the abdominal wall.
Can you understand that these appearances represent just about all of the “congenital” bowel diseases?
Answer: Yes. Can you name the disease with the arrow and progress counterclockwise?
GastrochisisOmphaloceleAtresia/stenosisMeckel diverticulumHirschsprungMalrotation
Understand the 5 different types of diarrhea, and the relationship between enterocolitis (inflammatory disease) and diarrhea (symptom)
If the purpose of a bowel mucosal epithelial cell is to absorb fluid, it does NOT absorb fluid when it is damaged.
An “osmotic” diarrhea means there are too many solutes in the lumen and therefore absorption is impaired, it is LEAST LIKELY to be associated with anatomic bowel mucosa damage.
Increased damage to an intestinal mucosal epithelial cell can result in EXUDATE from the mucosa TO the lumen. The condition is usually caused by gram positive enteric commensal bacteria of the gut (gut flora). Caecitis affects immunocompromised patients, such as those undergoing chemotherapy, patients with AIDS, kidney transplant patients, or the elderly
Malabsorption can be at the pancreas, bile, or bowel mucosal level.
Understand how BOTH a DECREASED or INCREASED transit time can be associated with diarrhea.
Rotavirus is the most likely cause of “stomach” flu, especially in kids.
Enterocytes are the most common type of intestinal cell and they ABSORB water and nutrients, so it is no surprise that watery diarrhea and malabsorption can be the sequelae when there is a disease of enterocytes.
“Traveller’s diarrhea” usually refers to E. coli infections, but also has a more generic connotation.
Which of these 3 conditions is most likely to produce histopathologic mucosal changes and blood in stools?? Ans: Enteroinvasive bacteria
What type of E. coli would be most likely to produce “hemorrhagic” diarrhea? Ans:Entero-invasive
Can a yersinia infection look like a maltoma? Ans: YES
Pseudomembranous colitis is usually also called “antibiotic induced” colitis. Why? (figure out this one yourself)
Bacterial overgrowth syndromes result in, and are caused by, L---O---N---G transit times
Helminths generally do not produce too much mucosal damage, BECAUSE “a successful parasite never kills its host”. This principle is also true in the business world and the usury trade. If you remember, the loan sharks rarely killed their victims, they just threatened to. Just like banks and credit card companies too.
Giardiasis in humans is caused by the infection of the small intestine by the CYST of a single-celled organism called Giardia lamblia. Giardiasis occurs worldwide with a prevalence of 20–30%[1] in developing countries. Additionally, Giardia has a wide range of human and other mammalian hosts, thus making it very difficult to eliminate. The CDC reports that in the US Giardia infects over 2.5 million people annually. This is one of the main reasons why people tell you “please do not drink the water”. PS: THE CYSTS CAN LIVE IN ICE TOO, SUCH AS SNO-CONES.
Like the Reed-Sternberg cell, this flagellate often gives you the feeling it is looking back at you when you look at it under the diagnostic microscope.
Like Diarrhea, malabsorption is a SYMPTOM, not a disease. As you can see it can be intricately related to diarrhea.
Malabsorption is a very LOGICAL concept.
Have you noted the trend for your favorite restaurant to offer gluten-free dishes, like pizza?
Mucosal (villous) flattening and chronic mucosal inflammation, Which one is more advanced? LEFT or RIGHT? Ans: The FLATTER one
Whipple's disease is a rare, systemic infectious disease caused by the bacterium Tropheryma whipplei
This is a classic examlpe of the malabsorption/diarrhea intimate relationship.
Idiopathic Inflammatory Bowel Disease
Idiopathic Inflammatory Bowel Disease.
WHY increased cancer risk? Initiation or Promotion?
Idiopathic Inflammatory Bowel Disease
Granulomas are NOT found in UC, distinct mucosal pseudopolyps are not found in CD
Pseudopolyp or fissure?
* NOT “dysplastic” in the classic sense of the word
Transmurally infarcted bowel is usually purple and paper thin.
Think of it as an AVM of the colonic submucosa!
A VERY common cause of GI bleeding.
Like varices, the ultimate cause is chronically elevated increased submucosal venous pressure, either from portal hypertension (much less likely), or ANYTHING which commonly causes chronically increased abdominal pressure, i.e., the same forces which are associated with abdominal hernias.
Like the esophagus “pseudo” means LACK of all 4 classical layers.
The perforating branches of the mesenteric artery branches are the weak links to be a setting for diverticuli!
When diverticuli are inflamed, you may not see a mucosa very easily.
Ileus is a disruption of the normal propulsive gastrointestinal motor activity from NON-mechanical mechanisms. Motility disorders that result from structural abnormalities are termed mechanical bowel obstruction. So if you think of the whole anatomy and physiology of peristalsis, ileus can be defined as any major problem in the whole scheme of things.
Can the whole classification of intestinal neoplasms be recalled by simply remembering the basic histology images with NO text? YES!
A villous pattern of growth, BY GEOMETRY ALONE, implies a faster growth rate than a tubular pattern of growth, hence a greater risk of malignant transformation.
What is more important?
How yucky the nuclei look?
If the glands have invaded into the submucosal stalk?
NOTE the various types of epithelial cells….this is the reason it is benign, i.e., NON monoclonal.
The key word here is “SERRATED”
TUBULAR adenoma, note how all the epithelial (glandular) cells look the same.
Villous adenomas behave more aggressively than tubular adenomas. They have a HIGHER rate of developing into frank adenocarcinomas than the “tubular” patterns.
For geometric reasons alone, the VILLOUS pattern of growth is faster than the TUBULAR pattern!
THREE types of hereditary or “familial” intestinal glandular tumors.
SMADs are intracellular proteins that transduce extracellular signals from TGF beta ligands to the nucleus where they activate downstream TGF-ß gene transcription
Whatever dietary carcinogenic influences are for the colon, the longer they hang around (transit time) the higher the risk!
Adjectives pathologists use.
Does a gland inside of a smooth muscle layer take all the guesswork out of agonizing whether that gland is benign or malignant? Ans: YES!
Does this look familiar? Like you’ve seen it before? Like stomach adenocarcinomas?
Does this look familiar? Like you’ve seen it before? Like stomach adenocarcinomas?
Does this look familiar? Like you’ve seen it before? Like stomach adenocarcinomas?
Signet ring cells are POORLY differentiated adenocarcinoma cells, and are OFTEN seen with linitis plastica.
Does this look familiar? Like you’ve seen it before? Like stomach adenocarcinomas?
Does this look familiar? Like you’ve seen it before? Like stomach adenocarcinomas?
To me, this looks very logical.
Often the DUKES classification may be used?
Why do you need neutrophils in the muscularis?
Ans: to differentiate from a peritoneal inflammation or luminal pus from another part of the bowel.
What is the white junk coating the surface? Answer: FIBRIN
The presence of neutrophils invading the muscularis is the diagnostic criteria needed to diagnosis or confirm, acute appendicitis!
A RUPTURED MUCINOUS CYSTADENOCARCINOMA can look exactly like benign pseudomyxoma peritoneii, but with (malignant) tumor cells present. Most adenomas/adenocarcnomas of the appendix are VERY mucinous!
You MUST think of the peritoneum ANATOMICALLY to understand its pathology, unless you have a photographic memory for power point bullets!