
Recomendados
Más contenido relacionado
La actualidad más candente
La actualidad más candente (20)
Destacado
Destacado (20)
Similar a Thorax and lungs
Similar a Thorax and lungs (20)
Más de mchibuzor
Más de mchibuzor (20)
Último
Último (20)
Thorax and lungs
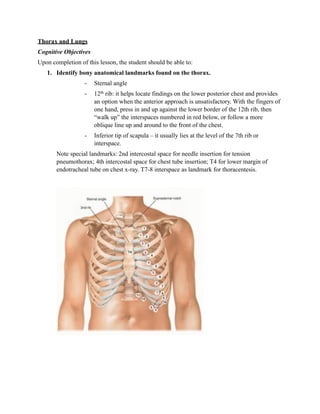
- 1. Thorax and Lungs Cognitive Objectives Upon completion of this lesson, the student should be able to: 1. Identify bony anatomical landmarks found on the thorax. - Sternal angle - 12th rib: it helps locate findings on the lower posterior chest and provides an option when the anterior approach is unsatisfactory. With the fingers of one hand, press in and up against the lower border of the 12th rib, then “walk up” the interspaces numbered in red below, or follow a more oblique line up and around to the front of the chest. - Inferior tip of scapula – it usually lies at the level of the 7th rib or interspace. Note special landmarks: 2nd intercostal space for needle insertion for tension pneumothorax; 4th intercostal space for chest tube insertion; T4 for lower margin of endotracheal tube on chest x-ray. T7-8 interspace as landmark for thoracentesis.
- 2. 2. Identify the following anatomical lines found on the thorax: a. Midsternal - drop vertically from suprasternal notch b. Midclavicular – drop vertically from midpoint of clavicle c. Anterior midaxillary – drop vertically from anterior axillary fold d. Posterior midaxillary – drop vertically from posterior axillary fold e. Vertebral – overlies the spinous processes of the vertebrae, drop vertically f. Scapular – drops from the inferior angle of scapula
- 3. 3. If given a drawing be able to identify the location of the three lobes of the right lung and two lobes of the left lung. (pg 287) Anteriorly, the Apex rises approximately 2 cm-4 cm above inner 3rd of clavicle. The lower border crosses 6th rib at midclavicular line & 8th rib at midaxillary line. Posteriorly, the lower border lies at level of T10 spinous process. On inspiration, it descends farther. Each lung divided roughly in half by oblique (major) fissure. This fissure approximated by a string from the T3 spinous process obliquely down and around the chest to the 6th rib at the midclavicular line. Right lung is divided by horizontal (minor) fissure. Anteriorly, this fissure runs close to 4th rib & meets oblique fissure in midaxillary line near 5th rib. It is divided into upper, middle, and lower lobes. Left lung has 2 lobes, upper and lower. • Supraclavicular—above the clavicles • Infraclavicular—below the clavicles • Interscapular—between the scapulae • Infrascapular—below the scapulae • Bases of the lungs—the lowermost portions • U p p e r, m i d d l e , a n d l o w e r l u n g f i e l d s Yo u m a y t h e n i n f e r w h i c h p a r t s o f t h e l u n g s a r e a ff e c t e d b y a n a b n o r m a l p r o c e s s . S i g n s i n t h e right upper lung field, for example, almost certainly originate in the right upper lobe. Signs in t h e r i g h t m i d d l e l u n g f i e l d l a t e r a l l y, h o w e v e r, c o u l d c o m e f r o m a n y o f t h r e e d i ff e r e n t l o b e s .
- 4. 4. Define tactile fremitus, provide a rationale for both increased and decreased tactile fremitus, and provide an example of a patient who would have increased and decreased fremitus. Feel for tactile fremitus. Patient speaking → Fremitus is palpable vibrations transmitted through bronchopulmonary tree to chest wall. Use either the ball (bony part of palm at base of fingers) or ulnar surface of your hand. Ask patient to repeat the words “99” or “1-1-1.” If fremitus is faint, ask patient to speak loudly / deeper. EXAMPLES OF ABNORMALITIES Fremitus decreased/ absent: voice is soft or when transmission of vibrations from the larynx to surface of the chest is impeded. Fremitus is usually decreased or absent over the precordium. Causes include: a) very thick chest wall b) obstructed bronchus c) COPD d) separation of pleural surfaces by * fluid (pleural effusion), * fibrosis (pleural thickening), * air (pneumothorax), * infiltrating tumor. Assessment of tactile fremitus. Compare both sides of the chest, using the ball or ulnar surface of your hand. When examining a woman, gently displace the breasts as necessary. Use one hand until you have learned the feel of fremitus. Some clinicians find using one hand more accurate. The simultaneous use of both hands to compare sides, however, increases your speed and may facilitate detection of differences.
- 5. 5. Describe the following abnormalities of the chest wall: a. Barrel Chest There is an increased anteroposterior (AP) diameter. This shape is normal during infancy, and often accompanies Aging & COPD. b. Funnel Chest (Pectus Excavatum) Note depression in the lower portion of the sternum. Compression of the heart and great vessels may cause murmurs. c. Pigeon Chest (Pectus Carinatum) The sternum is displaced anteriorly, increasing the anteroposterior (AP) diameter. The costal cartilages adjacent to the protruding sternum are depressed.
- 6. 6. Define percussion and compare and contrast the characteristics of the following five percussion notes: Percussion sets the chest wall and underlying tissues in motion, producing audible sound and palpable vibrations. Percussion helps you establish whether the underlying tissues are air-filled, fluid-filled, or solid. It penetrates only 5 cm to 7 cm into the chest, however, and will not help you to detect deep-seated lesions. Dullness - replaces resonance when fluid or solid tissue replaces air-containing lung or occupies the pleural space beneath your percussing finger. a. Tympany b. Resonance c. Hyperresonance –generalized hyperresonance may be heard over hyperinflated lungs of COPD or asthma. Unilateral hyperresonance suggest pneumothorax. d. Flat Intensity Pitch Duration Location e.g example Flatness Soft High Short Thigh Large pleural effusion Dullness Medium Medium Medium Liver Lobar pneumonia Resonance Loud Low Long Lung (healthy) Simple chronic bronchitis Hyperresonance Very loud Lower Longer None COPD, pneumothorax Tympany Loud High * Gastric air Large bubble pneumothorax 7. Compare and contrast the characteristics, normal location on exam, and the physiological rationale for the following breath sounds: a. Vesicular – soft and low pitched. Heard through inspiration and continue without pause through expiration. Fades away about 1/3 way through expiration. b. Bronchovesicular – inspiratory and expiratory sounds about equal in length. Detecting difference in pitch/intensity easier during expiration. c. Bronchial – louder and higher in pitch, with a short silence between inspiratory and expiratory sounds. Expiratory sounds are longer than inspiratory sounds. Duration Intensity Pitch of Locations expiratory expiratory sound sound Vesicular Inspiratory sounds last Soft Low Over most of longer than expiratory both lungs
- 7. Bronchovesicular Inspiratory/expiratory Intermediate Intermediate 1st/2nd interspace sounds equal Bronchial Expiratory sounds last Loud High Over manubrium longer than inspiratory Tracheal Inspiratory/expiratory Very loud High Over trachea in equal neck 8. Describe the characteristics of the following adventitious breath sounds, provide a physiological rationale for each, and identify a type of patient in which they may be commonly found. a. Crackles (rales) – discontinuous, intermittent, nonmusical. May be from abnormalities of lungs (pneumonia, fibrosis, early congestive heart failure) b. Wheezes – suggests partial airway obstruction from secretions, tissue inflammation, or foreign body. Wheezes suggest narrowed airway as in asthma, COPD, or bronchitis. Continuous, musical, prlonged, relatively high-pitched with hissing/shrill quality. c. Rhonchi – relatively low-pitched with snoring quality. Suggests secretions in large airways. 9. Define the following transmitted voice sounds and describe their significance when found on exam. a. Bronchophony – Ask the patient to say “ninety-nine.” Normally the sounds transmitted through the chest wall are muffled and indistinct. When sounds are louder, and clearer voice, this abnormality is known as Bronchophony. b. Egophony - Ask the patient to say “ee.” You will normally hear a muffled long E sound. When “ee” is heard as “ay,” an E-to-A change (egophony) is present, as in lobar consolidation from pneumonia. The quality sounds nasal. c. Whispered pectoriloquy – Ask the patient to whisper “ninety-nine” or “one-two- three.” The whispered voice is normally heard faintly and indistinctly, if at all. Louder, clearer whispered sounds are known as whispered pectoriloquy. 10. Compare and contrast the following physical findings noted on the exam of a patient with pneumonia (consolidation) versus pneumothorax: a. percussive note b. breath sounds c. adventitious sounds d. transmitted voice sounds ( tactile and vocal fremitus) 11. Describe the importance of the following symptoms of respiratory disease
- 8. a. Dyspnea – a nonpainful but uncomfortable awareness of breathing, commonly termed shortness of breath. Dyspnea commonly results from cardiac or pulmonary disease b. Chest pain – raises concern on heart disease, but also arise from structures of thorax and lung as well. Lung tissue has no pain fiber, so pain in lung condition such as pneumonia or pulmonary infarction arise from inflammation of adjacent parietal pleura. Chest pain may be due to myocardium (angina pectoris, MI), pericardium (pericarditis), aorta (dissecting aortic aneurysm), trachea and large bronchi (bronchitis), parietal pleura (pericarditis, pneumonia), chest wall (chostochondiritis, herpes zoster), esophagus (reflux esophagitis), neck/ gallbladder/stomach (cervical arthritis, biliary colic, gastritis). c. Wheezing – suggest partial airway obstruction from secretions, tissue inflammation, or a foreign body. d. Cough – reflex response to stimuli that irritate receptors in larynx, trachea, or large bronchi. These stimuli include mucus, pus, blood, dust, foreign bodies, and/ or even hot/cold air. Other causes include inflammation of respiratory mucosa, pressure or tension in air passages from a tumor, or enlarged peribronchial lymph nodes. e. Hemoptysis – coughing up blood from lungs. Blood or blood-streaked material may originate in mouth, pharynx, or GI tract. Clinical Objectives 1. Obtain a relevant history for complaints relating to the respiratory system, to include the history of present illness (HPI), relevant past medical history (PMH). social history (SH) and family history (FH) and review of system(s) (ROS) as outlined in Bickley and H&P Plus Booklet. 2. The student will demonstrate a complete and systematic examination of the lungs and thorax by completion of the following objectives: a. Demonstrate inspection of the chest noting respiratory rate and rhythm, deformities of chest wall, and presence of retractions. b. Demonstrate palpation of the chest wall noting tenderness or the presence of masses. c. Demonstrate chest expansion looking for symmetry of expansion. d. Demonstrate tactile fremitus noting symmetry. e. Demonstrate percussion of the anterior, posterior, lateral chest wall noting symmetry and percussive note. f. Demonstrate percussion of the diaphragmatic level. g. Demonstrate auscultation of the anterior, posterior, and lateral chest wall in 5 cm segments describing type of breath sounds and presence of adventitious sounds.
- 9. h. Demonstrate vocal fremitus by bronchophony, egophony, and whispered pectroriloquy. i. Record a complete respiratory exam using correct terminology.