

Recomendados
Más contenido relacionado
La actualidad más candente
La actualidad más candente (20)
Destacado
Destacado (20)
Similar a Shoulder
Similar a Shoulder (20)
Más de orthoprince
Más de orthoprince (20)
Último
Último (20)
Shoulder
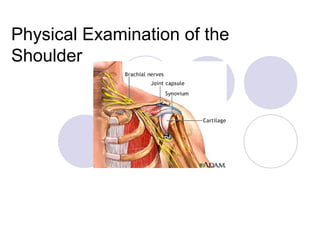
- 1. Physical Examination of the Shoulder
- 2. Examination of shoulder Anatomy History Inspection Palpation Range of Motion Special tests – Impingement tests Labral tests Instability tests Rotator Cuff tests Strength tests Acromio-clavicular joint tests Measurements Cervical Spine and Neurological Examination
- 3. Shoulder pain Common in all age groups Intrinsic disorder (85%) vs referred pain C-spine nerve impingement (disc herniation or spinal stenosis) Peripheral nerve entrapment distal to spinal column (long thoracic, suprascapular) Diaphragm irritation, intrathoracic tumors, and distension of Gleason’s capsule/gall bladder Myocardial ischemia Pancoast tumor
- 4. Review of shoulder anatomy
- 5. Review of shoulder anatomy Bones Scapula Clavicle Humeral head Posterior rib cage Joints Sternoclavicular Acromioclavicular Glenohumeral Scapulothoracic
- 6. Glenohumeral joint 25% humeral head surface in contact with glenoid Joint space thinning seen with OA
- 7. Glenohumeral joint Humeral head coverage increased to 75% with glenoid labrum
- 8. More shoulder anatomy Ligaments Coracoclavicular Acromioclavicular Glenohumeral Superior GH Middle GH Inferior GH Coracohumeral Subacromial bursa Subdeltoid bursa
- 9. Rotator cuff muscles Supraspinatus, infraspinatus, teres minor, subscapularis Form cuff around humeral head Keep humeral head within joint (counteract deltoid) Abduction, external rotation, internal rotation
- 10. Muscles of the Rotator Cuff The four major muscles of the rotator cuff rotate the humerus and properly orient the humoral head in the glenoid fossa (socket). The tendons of these four muscles merge, forming a cuff around the glenohumeral joint. Supraspinatus: abducts the humeral head and acts as a humeral head depressor Infraspinatus: externally rotates and horizontally extends the humerus Teres minor: externally rotates and extends the humerus Subscapularis: internally rotates the humerus
- 11. History Ask questions pertaining to the following: Chief complaint Mechanism of injury - Thrower, RTA,Thrower, RTA, sudden traction, repetitive overhead workersudden traction, repetitive overhead worker Unusual sounds or sensations Previous injury Previous injury to opposite extremity for bilateral comparison
- 12. History - PainHistory - Pain Type and location of pain or symptoms Onset of pain (traumatic, insidious)Onset of pain (traumatic, insidious) Location of painLocation of pain Alleviating/Aggravating factorsAlleviating/Aggravating factors Night painNight pain Pain/weakness overhead activitiesPain/weakness overhead activities
- 13. PainPain Where is the pain?(C4 or C5) How Long for? Other Joints? 1. Able to lie on that side? 2. Pain at rest? 3. Pain down the arm? (how far) The last 3 questions determine the irritability of the joint
- 14. Pain The shoulder is derived from the fifth cervical segment and therefore refers pain into the C5 dermatome. The acromio-clavicular joint is a C4 structure and refers pain into the C4 dermatome.
- 15. Pain The extent of reference is governed by a number of factors. The depth of the structure beneath the skin. The position of the structure within the dermatome. The severity of the lesion
- 16. Pain The shoulder is deep and proximal in the C5 dermatome, hence it can potentially refer pain a great distance. Conversely the acromio-clavicular joint is a superficial structure at the distal end of the dermatome causing it to give rise to accurate, local pain
- 17. Pain Typically pain of gleno-humeral origin is felt in the upper arm, often at the insertion of the deltoid. Severe shoulder problems can cause pain to radiate as far as the radial side of the wrist. Other potential sources of pain at the shoulder need to be eliminated (angina, pleuritic pain or neck pain.)
- 18. Pain Pain behaves in a predictable manner. There are several 'rules of referral' Pain is generally referred distally. Pain is felt deeply. Pain does not cross the mid—line. Pain may occupy any part of the dermatome. Pain is felt segmentally.
- 19. Pain The exception to the rules of referred pain is the dura mater which will give rise to extrasegmental referred pain.
- 20. Painful Arc This is not a diagnosis but a localising sign. There are 4 common causes of a painful arc at the shoulder joint. All involve soft tissues being pinched between the humerus and the underside of the acromion.
- 21. Painful Arc These are: supraspinatus (pain on resisted abduction) infraspinatus (pain on resisted lateral rotation). subscapularis (pain on resisted medial rotation). sub-acromial bursa (pain at extremes of all passive ranges
- 22. Examination of the Shoulder 1. Observe the whole patient, front and back. 2. Observe the shoulder. 3. Observe the axilla. View from rear with patient standing straight and look for lateral symmetry, swelling, position of scapula and signs of muscle wasting.
- 23. Inspection Posture: Cervical lordosis, thoracicPosture: Cervical lordosis, thoracic kyphosis, and rounded shoulderskyphosis, and rounded shoulders Relative elevation or depression shoulderRelative elevation or depression shoulder Muscle atrophyMuscle atrophy Prominent AC jointProminent AC joint Scapula motion during arm elevationScapula motion during arm elevation Active/Passive range of motionActive/Passive range of motion
- 24. Inspection Visible facial expressions of pain Swelling, deformity, abnormal contours, or discoloration Does the arm hang and swing, or does he hold or splint the arm? Overall position, posture, and alignment Muscle development—are there areas of muscular atrophy? Bilateral comparison of acromions, SC joints, inferior border of scapula, and scapular spine Is the inferior tip of scapula level with T7 and the superior medial ridge level with T2?
- 25. Observe shoulder abduction from in front and behind, through the entire range of movement. Note the presence of difficulty in initiation or a painful arc.
- 26. Palpation Bilaterally palpate for pain, tenderness, and deformity over the following: SC joint, clavicle, AC joint, acromion, coracoid process, subacromial bursa, greater tuberosity, lesser tuberosity, bicipital groove Spine, superior and inferior angles of scapula, lower cervical and upper thoracic spinous processes
- 27. Palpation Rotator cuff insertion Sternocleidomastoid, pectoralis Biceps tendon and muscle Trapezius, rhomboid, latissimus dorsi, serratus anterior Axillary structures
- 28. Range of Motion Tests conducted both actively and passively The reason for this is that if the patient is experiencing pain, he/she may restrict movement. Furthermore, the opposing limb should be examined in an identical fashion in order to evaluate bilateral symmetry.
- 29. External Rotation patient is positioned sitting and the elbow is flexed 90 degrees. While the elbow is held against the patient's side, the examiner externally rotates the arm as permitted.
- 30. Internal Rotation The patient should be positioned sitting. Again with the elbows at the patient's side, the examiner should raise the thumb up the spine, and record the position in relation to the spine (reaching T7 is normal, unless bilateral symmetry is observed).
- 31. Internal Rotation at 90 degrees of Forward flexion The patient is positioned sitting with the elbow and shoulder supported to prevent muscle contraction. The arm is at 90 degrees with the fingers pointing downward and palm facing posteriorly. The examiner attempts to rotate the forearm posteriorly as far as possible.
- 32. Forward flexion The arm is kept straightened and brought upward through the frontal plane, and moved as far as the patient can go above his head. Note: for recording purposes, 0 degrees is defined as straight down at the patient's side, and 180 degrees is straight up.
- 33. Shoulder Abduction: Active Test The arm is again kept straightened, while raised and abducted. Observe the twisting of hand -- facing outward, not forward, as in forward flexion. The ROM is measured in degrees as decribed for forward flexion. As pictured, this test is being done actively by the patient, but may be performed by the examiner as well.
- 34. Other movements Extension-with arm by the patient’s side, lift the arm back wards as far as possible. Adduction-draw the arm across the anterior chest wall as far as possible.
- 35. Functional examination- Thirteen tests: Bilateral elevation through abduction:— pain? / R.O.M? Passive elevation:- pain? / R.O.M? / end feel? Painful ARC:— (active elevation, encourage beyond pain) Passive abduction:- fix scapula, cf other side Passive lat. rotn:— fix other shoulder R.O.M? / end feel? Passive med. rotn:- fix other shoulder R.O.M? / end feel? Resisted adduction:- (pec major, lat dorsi, teres maj, teres min) Resisted abduction:- (SUPRASPINATUS, deltoid) Resisted lateral rotation:- (INFRASPINATUS, teres minor) Resisted medial rotation:- (SUBSCAPULARIS, P.macj. L.Dor. T.maj) Resisted elbow flexion:- (BICEPS long head) Resisted elbow extension:- (SUB ACROMIAL BURSA, TRICEPS) Passive horizontal adduct ion:- (A-C joint, subscapularis)
- 36. Special TestsSpecial Tests A variety of tests have been described forA variety of tests have been described for examination of the shoulderexamination of the shoulder A positive test is usually associated withA positive test is usually associated with pain in a specific location for each testpain in a specific location for each test No single test is diagnostic, but several testsNo single test is diagnostic, but several tests together along with the history is usuallytogether along with the history is usually very accurate at locating the source ofvery accurate at locating the source of pathologypathology
- 37. Special tests Impingement tests Labral tests Instability tests Rotator Cuff tests Strength tests Acromio-clavicular joint tests
- 38. Tests Used in Shoulder Evaluation and Significance of Positive Findings Test Maneuver Diagnosis suggested by positive result Apley scratch test Patient touches superior and inferior aspects of opposite scapula Loss of range of motion: rotator cuff problem Neer's sign Arm in full flexion Subacromial impingement Hawkins' test Forward flexion of the shoulder to 90 degrees and internal rotation Supraspinatus tendon impingement
- 39. Tests Used in Shoulder Evaluation and Significance of Positive Findings Test Maneuver Diagnosis suggested by positive result Drop-arm test Arm lowered slowly to waist Rotator cuff tear Cross-arm test Forward elevation to 90 degrees and active adduction Acromioclavicular joint arthritis Spurling's test Spine extended with head rotated to affected shoulder while axially loaded Cervical nerve root disorder
- 40. Tests Used in Shoulder Evaluation and Significance of Positive Findings Test Maneuver Diagnosis suggested by positive result Apprehensi on test Anterior pressure on the humerus with external rotation Anterior glenohumeral instability Relocation test Posterior force on humerus while externally rotating the arm Anterior glenohumeral instability Sulcus sign Pulling downward on elbow or wrist Inferior glenohumeral instability
- 41. Tests Used in Shoulder Evaluation and Significance of Positive Findings Test Maneuver Diagnosis suggested by positive result Yergason test Elbow flexed to 90 degrees with forearm pronated Biceps tendon instability or tendonitis Speed's maneuver Elbow flexed 20 to 30 degrees and forearm supinated Biceps tendon instability or tendonitis "Clunk" sign Rotation of loaded shoulder from extension to forward flexion Labral disorder
- 42. Impingement SignsImpingement Signs Neer (maximal forward flexion)Neer (maximal forward flexion) Hawkins (90o flexion, internal rotation,Hawkins (90o flexion, internal rotation, adduction)adduction)
- 43. Neer's Test (Neer's impingement sign ) is elicited when the patient's rotator cuff tendons are pinched under the coracoacromial arch. The test is performed by placing the arm in forced flexion with the arm fully pronated. The scapula should be stabilized during the maneuver to prevent scapulothoracic motion. Pain with this maneuver is a sign of subacromial impingement.
- 44. Hawkins' Test performed by elevating the patient's arm forward to 90 degrees while forcibly internally rotating the shoulder. Pain with this maneuver suggests subacromial impingement or rotator cuff tendonitis. One study found Hawkins' test more sensitive for impingement than Neer's test.
- 45. Hawkin's Test Position the patient standing with the shoulder abducted 90 degrees, and internally rotate the forearm. The presence of pain with movement is indicative of possible pathology
- 46. Labral TestsLabral Tests RelocationRelocation Active Compression (O’Brien’s)Active Compression (O’Brien’s) Abduction external rotationAbduction external rotation Load and shiftLoad and shift ShearShear Anterior SlideAnterior Slide Clunk SignClunk Sign
- 47. InstabilityInstability ApprehensionApprehension SulcusSulcus RelocationRelocation Load and shiftLoad and shift
- 48. 'Clunk' Sign Glenoid labral tears are assessed with the patient supine. The patient's arm is rotated and loaded (force applied) from extension through to forward flexion. A "clunk" sound or clicking sensation can indicate a labral tear even without instability.
- 49. Drawer Test The patient is seated with the forearm resting on the lap and the shoulder relaxed. The examiner stands behind the patient. One of the examiner's hands stabilizes the shoulder girdle (scapula and clavicle) while the other grasps the proximal humerus. These tests are performed with (1) a minimal compressive load (just enough to center the head in the glenoid) and (2) with a substantial compressive load (to gain a feeling for the effectiveness of the glenoid concavity).
- 50. Drawer Test Starting from the centered position with a minimal compressive load, the humerus is first pushed forward to determine the amount of anterior displacement relative to the scapula. The anterior translation of a normal shoulder reaches a firm end-point with no clunking, no pain and no apprehension. A clunk or snap on anterior subluxation or reduction may suggest a labral tear or Bankart lesion.
- 51. Drawer Test The test is then repeated with a substantial compressive load applied before translation is attempted to gain an appreciation of the competency of the anterior glenoid lip. The humerus is returned to the neutral position and the posterior drawer test is performed, with light and again with substantial compressive loads to judge the amount of translation and the effectiveness of the posterior glenoid lip, respectively.(Silliman and Hawkins, 1993)
- 52. InstabilityInstability ApprehensionApprehension SulcusSulcus RelocationRelocation Load and shiftLoad and shift
- 53. Apprehension TestHave the patient in the supine position, with the arm abducted 90 degrees. Rotate the shoulder externally by pushing the forearm posteriorly. If patient feels instability, they typically will balk when the test is performed.
- 54. Apprehension Test The anterior apprehension test is performed with the patient supine or seated and the shoulder in a neutral position at 90 degrees of abduction. apply slight anterior pressure to the humerus (too much force can dislocate the humerus) and externally rotates the arm. Pain or apprehension about the feeling of impending subluxation or dislocation indicates anterior glenohumeral instability.
- 55. Relocation Test The relocation test is performed immediately after a positive result on the anterior apprehension test. With the patient supine, the examiner applies posterior force on the proximal humerus while externally rotating the patient's arm. A decrease in pain or apprehension suggests anterior glenohumeral instability.
- 56. Sulcus Sign With the patient's arm in a neutral position, pull downward on the elbow or wrist while observing the shoulder area for a sulcus or depression lateral or inferior to the acromion. The presence of a depression indicates inferior translation of the humerus and suggests inferior glenohumeral instability remember that many asymptomatic patients, especially adolescents, normally have some degree of instability.
- 57. Rotator CuffRotator Cuff Lift-offLift-off Napoleon (belly push)Napoleon (belly push) Whipple (resisted elevation with cross bodyWhipple (resisted elevation with cross body adduction)adduction) External rotation arm at sideExternal rotation arm at side (infraspinatus)(infraspinatus) Empty can (supraspinatus)Empty can (supraspinatus)
- 59. Drop-Arm Test A possible rotator cuff tear can be evaluated with the drop-arm test. This test is performed by passively abducting the patient's shoulder, then observing as the patient slowly lowers the arm to the waist. Often, the arm will drop to the side if the patient has a rotator cuff tear or supraspinatus dysfunction. The patient may be able to lower the arm slowly to 90 degrees (because this is a function mostly of the deltoid muscle) but will be unable to continue the maneuver as far as the waist.
- 60. Rotator cuff strength testing Supraspinatus “Pour out a Coke” Infraspinatus and teres minor “Act like a penguin” Subscapularis “Scratch your back”
- 61. Strength Tests Position the patient sitting, with his arms at his sides and elbows at 90 degrees. It is important to maintain the elbow positioning at the sides while the external rotation is attempted by the patient (the examiner applies internal resistance). External Rotator Cuff (RC) Strength
- 62. Internal RC Strength Same as above, but the patient is attempting to rotate internally (and examiner resisting externally).
- 63. Supraspinatus Strength The patient is positioned sitting with arms straight out, elbows locked, thumbs down, and arm at 30 degrees (in scapular plane). The patient should attempt to abduct his arms against the examiner's resistance.
- 64. Acromioclavicular (AC) Joint Testing Palpation of AC Joint The patient's arm is kept at his side and the examiner palpates the AC joint for discomfort/pain and gapping.
- 65. Cross-Arm Horizontal Adduction Test The patient places his hand on the opposite shoulder, while the examiner exerts force horizontally. Again, the presence of pain indicates possible pathology.
- 66. Cross-Arm Test Patients with acromioclavicular joint dysfunction often have shoulder pain that is mistaken for impingement syndrome. The cross-arm test isolates the acromioclavicular joint. The patient raises the affected arm to 90 degrees. Active adduction of the arm forces the acromion into the distal end of the clavicle . Pain in the area of the acromioclavicular joint suggests a disorder in this region.
- 67. Cervical Spine and Neurologic ExamCervical Spine and Neurologic Exam Cervical spine range of motionCervical spine range of motion Hyperextension of cervical spineHyperextension of cervical spine Comparison of bilateral upper extremityComparison of bilateral upper extremity strength, sensation, and reflexesstrength, sensation, and reflexes Spurling’s maneuverSpurling’s maneuver
- 68. Spurling's Test In a patient with neck pain or pain that radiates below the elbow, a useful maneuver to further evaluate the cervical spine is Spurling's test.
- 69. Spurling's Test The patient's cervical spine is placed in extension and the head rotated toward the affected shoulder. An axial load is then placed on the spine Reproduction of the patient's shoulder or arm pain indicates possible cervical nerve root compression and warrants further evaluation of the bony and soft tissue structures of the cervical spine.
Notas del editor
- Normal shoulder movement. Also, character of the pain does not change with movement of the shoulder.
- Sternoclavicular, acromioclavicular, glenohumeral, and scapulothoracic joints. Thin capsule. Subacromial bursa. Rotator cuff tendons attach to humeral tuberosities.
- Supraspinatus – abduction (also with deltoid). Infraspinatus and teres – external rotation. Subscapularis – internal rotation.