Finalists of the 2023 Business Case for Healthcare Quality

Improvements in healthcare quality increase patient safety and satisfaction, positively impacting the reputation of a facility. However, these may also require resources: more budget, effort, or time – either to employ and train new staff or to invest in equipment and hospital infrastructure. But what is the impact on the bottom line? There is little evidence publicly on how quality influences the financial health of institutions. As a result, hospitals often lack the resources they need to make data-based decisions about quality programs. In order to provide additional evidence, IFC launched the “Business Case for Healthcare Quality” contest. The goal: to present real-life cases from hospitals around the world that successfully used quality to improve their business. Participating institutions that displayed a strong understanding of the business case for healthcare quality and provided a measurable impact collaborated with the IFC IQ-Health program to produce the 2023 Business Case for Healthcare Quality Highlights. IFC gleaned further insights by conducting interviews with top leadership, as well as the quality practitioners who implemented new programs. About IFC IQ-Healthcare Responding to global gaps in healthcare competence, IFC IQ-Healthcare —with the IQ standing for Improving Quality—helps health providers improve patient safety, align practices with global quality standards, and build safe health infrastructure. To date, the IFC IQ-Healthcare program has helped more than 130 hospitals and clinics in nearly 20 countries. Over 6,000 healthcare professionals benefited from IFC open resources: a webinar series and self-paced training on healthcare quality and patient safety. Learn More at https://www.ifc.org/iqhealth

Recomendados
Más contenido relacionado
Similar a Finalists of the 2023 Business Case for Healthcare Quality
Similar a Finalists of the 2023 Business Case for Healthcare Quality (20)
Más de International Finance Corporation
Más de International Finance Corporation (10)
Último
Último (20)
Finalists of the 2023 Business Case for Healthcare Quality
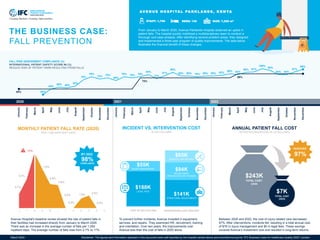
- 1. 2.7% 5.7% 11% 7.8% 4.8% 4.6% 0.0% 0.0% 1.9% 2.5% 0.0% J F M A M J J A S O N D MONTHLY PATIENT FALL RATE (2020) PER 1,000 INPATIENT DAYS 30% 45% 50% 48% 53% 70% 78% 72% 75% 68% 78% 75% 78% 84% 73% 81% 90% 80% 80% 78% 80% 80% 82% 86% 84% 90% 91% 100% 95% 84% 84% 91% 98% 45% 75% 86% January February March April May June July August September October November December January February March April May June July August September October November December January February March April May June July August September October November December Avenue Hospital's baseline review showed the rate of patient falls in their facilities had increased sharply from January to March 2020. There was an increase in the average number of falls per 1,000 inpatient days. The average number of falls rose from 2.7% to 11%. THE BUSINESS CASE: FALL PREVENTION FALL RISK ASSESSMENT COMPLIANCE (%) INTERNATIONAL PATIENT SAFETY SCORE #6 (%) REDUCE RISK OF PATIENT HARM RESULTING FROM FALLS AV E N U E H O S P I TA L PA R K L A N D S , K E N YA From January to March 2020, Avenue Parklands Hospital observed an uptick in patient falls. The hospital quickly mobilized a multidisciplinary team to conduct a thorough root-case analysis. After identifying several problem areas, they designed and implemented a three-year program of quality improvements. The data below illustrates the financial benefit of these changes. 2020 2021 2022 To prevent further incidents, Avenue invested in equipment, services, and repairs. They examined HR, recruitment, training, and orientation. Over two years, the improvements cost Avenue less than the cost of falls in 2020 alone. Between 2020 and 2022, the cost of injury-related care decreased 97%. After interventions, incidents fell, resulting in a total annual cost of $7K in injury management and $0 in legal fees. These savings covered Avenue’s investment cost and resulted in long-term returns. 98% COMPLIANCE BY 2022 97% REDUCED ANNUAL PATIENT FALL COST AFTER INTERVENTION, IN US DOLLARS $243K TOTAL COST (2020) $7K TOTAL COST (2022) BEDS: 130 STAFF: 1,700 SIZE: 7,229 m2 COST OF FALLS IN 2020 INTERVENTION COST 2020-2022 INCIDENT VS. INTERVENTION COST IN US DOLLARS $188K LEGAL FEES $55K INJURY MANAGEMENT $141K STRUCTURAL ADJUSTMENTS $94K RECRUITMENT ORIENTATION AND TRAINING $65K SERVICES AND REPAIRS March 2024 Disclaimer: The figures and information depicted in this document were self-reported by the hospital named above and submitted during the “IFC Business Case for Healthcare Quality 2023” contest.
- 2. What problem did the hospital face? In early 2020, our hospital recorded a significant increase in falls. During a three-month period, the fall rate increased from 2.7% to 11% per 1,000 patient days. Three of these cases were sentinel events, resulting in serious injuries. Apart from the human tragedy, they cost the organization $190,000 in compensation payments. Why were patients falling? After a root cause analysis, we identified several factors related to falls, specifically with infrastructure. Our floors were slippery, especially the bathrooms. There were no guardrails in the hallways, no alarms at the bedside or in the bathrooms. Our policies and procedures needed attention. Another problem included staffing. We had to work on nursing hours per patient day. The number of nurses was inadequate given the kind of attention patients needed. What was done to alleviate the situation? There were many mitigation measures, but a few important ones included improving the hospital’s infrastructure. Also, we made it easy for staff to identify high-risk patients with a yellow wristband so that when they appeared at any point of care delivery, staff would see it and pay more attention to fall prevention measures. We also instituted new policies and procedures and educated families on risks. What role did staff ratio play in falls? We compared the number of falls when we had very low nursing hours per patient days from 4.5 hours previously to 9.5 hours today. We tallied statistics every day and reviewed them monthly to make decision data. Figures do not lie. Things improved and we reduced the falls to almost zero. Should we aim for zero falls or is it normal for patients to fall anyway? Falls still happen even when measures have been put in place. For us, if there was a fall despite our best efforts, it was much less severe. After every incident, it is very important to identify where things went wrong. In our case, most of the recent falls happened when we relaxed a little bit. For example, when we hired part-time workers to substitute staff taking vacation. What challenges did you face? Introducing and implementing change was not easy, especially as the program spanned three years. I was a new staff member determined to change the culture and behavior of staff who worked there for many years. They were used to doing things in a particular way. I knew that I needed to be strategic. What advice can you give to quality teams to obtain financial support from top leadership? In my experience, the only way to effectively communicate with leadership is through data. It must be demonstrated and linked. It must also be continuously tracked and monitored to show the costs that will rise if there is nonconformity. Who were the important key stakeholders needed to achieve success? When it comes to healthcare quality, the nursing team is the driving force. They are crucial to pushing policy agendas because they are the majority in any healthcare facility, and they are the ones who spend most of their time with patients. “Figures do not lie. Things improved and we reduced the falls to almost zero.” ___________________ Do patients appreciate these efforts and that the hospital is safer? Yes. In fact, we see clear evidence of this on social media. From a quality perspective, our Net Promoter Score (NPS) is public. We embrace transparency. We have a live screen where patients can air their concerns, and we address them positively as they happen. This is further demonstrated by the fact that we discuss incidents with patients. What is next for Avenue Parklands? We have many ongoing projects. We are consistently collecting data to identify areas that need improvement. One of our current focus areas is the turnaround time for admission and discharge. Patients have highlighted this as a significant pain point. We are also passionate about reducing maternal mortality rates and have made significant progress in this area. Any last words of wisdom? Maintaining quality in a hospital is not a one-time task. It requires continuous effort and improvement. Quality is never delegated. It is everyone’s responsibility. HER LIFELONG MISSION: TO IMPACT HEALTHCARE QUALITY Penina Kirea of Avenue Parklands describes how her mother’s passing in childbirth fueled her commitment to improve healthcare quality for all. Penina Kirea Group Chief Nursing Officer and Head of Quality Avenue Healthcare The IFC Business Case for Healthcare Quality contest is sponsored by IFC’s IQ-Healthcare program in partnership with the governments of Japan, Norway, and the Netherlands. Contact Us www.ifc.org/iqhealth ifc_healthcare@ifc.org Scan code below to join our community of practice, or visit http://bit.ly/3ZYt1PO How implementing a fall prevention program directly impacted Avenue Hospital’s operations.
- 3. MONTH 1 MONTH 2 MONTH 3 MONTH 4 Patients began canceling their annual diabetes care memberships, which adversely impacted patient access in addition to business results. Implementing software that used clinical guidelines for medication, significantly decreased cancellations. C L I N I C A S D E L A Z U C A R , M E X I C O The software intervention was implemented when Azucar had just 15 clinics. Since then, it has continued to be an important quality control tool as new service areas have opened. Today, the EHR is used in Azucar’s 37 clinics across Mexico. GROWTH IN NUMBER OF CLINICS AFTER INTERVENTION 2x SERVICE AREAS STAFF: 600 SIZE: 250 m2 CLINICS: 37 Clinicas del Azucar, Mexico's largest diabetes and hypertension clinic network, identified numerous medication errors causing patient dissatisfaction, appointment cancellations, and treatment discontinuation. To address this, the hospital implemented medication guidelines and electronic health record (EHR) improvements, empowering doctors to improve patient care. The following data highlights the financial benefits of these changes. BEFORE INTERVENTION AFTER INTERVENTION THE BUSINESS CASE: TREATMENT GUIDELINES COST OF PATIENT CANCELLATIONS IN # OF CANCELLATIONS ENHANCED COMPLIANCE % PRESCRIBED MEDICATIONS OUTSIDE GUIDELINES In the initial week of measurement, 13% of medication was outside the guidelines. After four months, this percentage was significantly reduced to 2%. This reduction in medication errors contributed to a noteworthy decrease in patient cancellations and complaints. 13% MONTH 1 2% MONTH 4 TREATMENT GUIDELINES INTRODUCED EHR SYSTEM DEPLOYED BETTER PATIENT SAFETY COST OF CARE DECREASES ENHANCED DOCTOR ENGAGEMENT HIGHER PATIENT SATISFACTION BETTER PATIENT RETENTION MORE DEMAND FOR SERVICES BUSINESS EXPANSION FEWER ERRORS COMPLIANCE INCREASES REDUCED ERRORS PAID BACK IN 1 MONTH $360K SAVINGS PER YEAR $20K INVESTMENT 100 CANCELATIONS AVOIDED PER MONTH March 2024 Disclaimer: The figures and information depicted in this document were self-reported by the hospital named above and submitted during the “IFC Business Case for Healthcare Quality 2023” contest.
- 4. What problems did the clinics face? We were losing patients; they were canceling their diabetes care memberships. Why were they canceling? Patients were having side effects. Others couldn’t afford the care. The diabetes medication was also not tailored to their needs. We found that doctors would recommend the same prescription for everyone, especially for low-income patients. We discovered a hiccup in the way diabetes patients are treated everywhere. Although doctors follow treatment guidelines, they prescribe based on averages. But people vary greatly. If you look at the ADA and global guidelines, they are generic and almost the same for every patient, whether married, single, divorced, male, female, 40, or 60 years old. What was done to alleviate the situation? We built an electronic system that used algorithms to open or close medications. Using a software platform provided protection and standardization. Following a standard is always safer because it excludes the human factor. We had concerns about the type of medication and the costs and whether doctors were being pressured by the industry to push a specific medication. Of course, the doctor had the flexibility to override recommendations and prescribe whatever they needed to. Did doctors still have the final say? We needed to continue to give the doctor the flexibility to choose what to prescribe. However, the system would say to this patient, “Only consider this list.” So, when the doctor prescribes something outside that list, the system automatically first says, "You are prescribing something outside the recommendation," and then asks why. The doctor needed to justify a different medication. As you implemented the new medication guideline software, what happened? It was very interesting. We could see what was happening in all the clinics at the same time. There was a lot of variation in treatment recommendations because doctors were often overriding the software’s suggested prescriptions. Some doctors said the patient requested a medication they thought was better, but a few weeks later the patient would come back. Having not taken the medication, they were afraid to tell the doctor this happened because they couldn't afford it. The doctors complied with most of the guidelines but reducing this trend took a different approach. Doctors with high compliance scores were named mentors for other doctors. We implemented this a few years ago, and it has allowed us to quickly scale the number of clinics. What other supports did you put in place? We have a patient support center, which is a call center that reaches out to the patients on certain days to ask how they are feeling, whether the amount and cost of the medication are okay, and whether they understand the medication change correctly. As a leader, do you have any tips for those implementing similar technology? Build a culture of technology process improvement from the beginning. That is the only way to enable delivery at low cost to “Build a culture of technology process improvement from the beginning.” __________________ millions. Because we started from scratch, we were able to set the tone from early on. It is very important for the CEO to consistently convey the message. It is critical to define the strategy and the type of company you are creating, and have executive leadership agree on that. Switching gears, on a personal note, what compelled you to disrupt the system? I had spent years applying process improvements to chronic care around the world. The issue became very personal when it came to researching diabetes, a disease my mother battled for ten years. She was exhausted from going from doctor to doctor, multiple doctors who gave conflicting advice. She didn’t want treatment anymore, even if she died. I was shocked. That was my aha moment. I realized diabetes care was broken everywhere. I launched Clinicas del Azúcar to create highly efficient diabetes clinics so patients could receive seamless treatment. I applied all my years of experience with a mission: to transform care by creating standardized one-stop shops around the country. DISRUPTING DIABETES CARE: AN ENTREPRENEUR’S ULTIMATE GOAL In an interview with IFC, Javier Lozano, CEO of Clinicas del Azúcar, describes how gaps in his mother’s diabetes treatment propelled him to disrupt the entire industry. Javier Lozano CEO CLINICAS DEL AZÚCAR How implementing new medication protocols dramatically improved patient retention and created a reliable system for quality and patient safety. The IFC Business Case for Healthcare Quality contest is sponsored by IFC’s IQ-Healthcare program in partnership with the governments of Japan, Norway, and the Netherlands. Contact Us www.ifc.org/iqhealth ifc_healthcare@ifc.org Scan code below to join our community of practice, or visit http://bit.ly/3ZYt1PO
- 5. 72% OVERALL -5% OVERALL Facilities Growth Patient Growth Before Intervention After Intervention 2017 2018 2019 2020 2021 2022 The Ministry of Health estimates only 40% of care delivered in Kenya meets national recommendations. Penda Health was at a similar level before addressing quality improvements. Now, they are one of the highest-performing facilities in the country. P E N DA H E A LT H , K E N YA The plan, implemented over four years, quadrupled Penda’s physical footprint. More importantly, its patient volume increased tenfold while it continued to improve customer satisfaction and affordability for low-income patients. GROWTH IN NUMBER OF CLINICS BEFORE AND AFTER INTERVENTION 10X PATIENT GROWTH Penda Health leads in offering high-quality primary care. They primarily serve lower- income markets in Kenya. Standardizing IT and clinical support mechanisms allowed for the quicker rollout of new clinics. It also positively impacted workflow, as staff quickly aligned to the new systems. THE BUSINESS CASE: STANDARDIZING PRIMARY CARE BEST IN CLASS PERFORMANCE COMPARED TO MINISTRY OF HEALTH AVERAGES IMPROVED EFFICIENCY AFTER LAUNCHING EHR Clinical decision support allowed Penda to quickly and easily scale its quality systems across new clinics – allowing new medical staff to be quickly trained and onboarded. Clinicians used the EHR in 90% of visits and adhered to its recommendations more than 75% of the time. STAFF: 350 FACILITIES: 19 BEDS: 130 EHR FULLY IMPLEMENTED ($250,000) CDSS LAUNCH & TRAINING ($30,000) IMPROVEMENTS & ADDITION OF 300+ CONDITIONS 90% UTILIZE CLINICAL DECISION SUPPORT 75% ADHERE TO RECOMMENDATIONS CDSS FRAMEWORK DEVELOPED EFFICIENCY GROWTH EHR UTILIZATION 90% COMPLIANCE 40% COMPLIANCE NATIONAL GUIDELINE COMPLIANCE NET PROMOTER SCORE 4X CLINICS March 2024 Disclaimer: The figures and information depicted in this document were self-reported by the hospital named above and submitted during the “IFC Business Case for Healthcare Quality 2023” contest. IMPROVED REFERRAL SYSTEM
- 6. What problem did the company face? Standardization was lacking which complicated operations in several areas. For instance, healthcare providers were recommending treatments outside of the national treatment guidelines. This led to inconsistencies in care and complicated our pharmaceutical supply chain. At the time, our pharmacy had 1,400 SKUs. Using an EHR with clinical decision support allowed us to standardize clinic operations and patient flow, so we could frontload processes in very busy clinics. Ultimately, reducing costs, which allowed us to expand services to even more patients. How does the setting impact the amount of standardization required? In the US, doctors typically treat about 20 conditions over and over, because we have a high degree of specialization. In that setting, clinical decision support for those experts is not needed. At Penda, in a week they are vaccinating children, treating motorcycle accidents, seeing chronic illnesses, delivering babies, and taking care of pregnant moms. The spectrum is truly massive and the multitasking that each clinician does requires this support. Standardization actually makes everyone much safer. What were a few important things that you got right? Changing culture is incredibly important, especially when implementing clinical decision support. A lot of people think technology is the most important thing, but it's not. Operationally, we said, let’s not go straight to standardizing treatment protocols for 300 conditions, let's start with 20. We did that for about six months. We also launched a big change management effort and made infographics and shared them on WhatsApp. We put posters up, conducted Zoom town halls, and explained why we were standardizing. We bought cakes and celebrated. It is critical to have champions. Who helped you through this process? The group that led the roll out consisted of a clinical quality team. They would visit different facilities and involve staff and managers. If I could do it over again, I would involve frontline staff even more initially. How did you help the finance department to see the value of approving these expenses? Penda is investor-backed, so we have unlocked support for scalable growth. Investments in technology make sense. The good thing is, electronic health records are becoming affordable and there are free options. Did success depend on technology solutions, such as EHRs? Yes. My advice is to invest fully in EHR first, then build in digital support. This is the hardest part but if you want scalable quality, you must have it. Once you installed the new clinical system, did you notice any reduction in the number of incidents or other improvements? Yes. We now have a really robust system that compiles a patient safety report every other day or so. We're very much on top of the safety “EHRs are becoming vastly more affordable and there are lots of free options” ____________________ issues. The wrong treatment of a diagnosis has gone way down. The beauty of clinical decision support is that it is a cloud-based record. No matter which facility of Penda you're at, it's the same record, notes and clinical decision support tools. This has improved consistency. The system allows for communication through the medical record that all doctors can access. Has the outside world noticed? Yes. There has been a lot of interest in what Penda has done with clinical decision support from other Chief Medical Officers. They are our competitors, but they're also our friends and colleagues within the ecosystem and we've been talking very openly about what we've done. Everyone is interested in doing it. So basically, with this initiative, we were the first, so we actually impacted the market as well. The rest of the market will follow after us. The barrier is that so few healthcare organizations that provide outpatient services in Kenya have electronic records. If you're not actually paperless then you can't implement clinical decision support even if you want to. Making a commitment to become fully digital is key. A DOCTOR’S DREAM: TO STANDARDIZE OPERATIONS Robert spoke with the IFC from his office in Nairobi about his journey standardizing operations and how using electronic health records (EHRs) has unlocked growth at scale. Dr. Robert Korom Chief Medical Officer at Penda Health How technology solutions standardized clinical decisions, led to better quality outcomes, and reduced costs. The greatest outcome of this? The ability to reach more patients. The IFC Business Case for Healthcare Quality contest is sponsored by IFC’s IQ-Healthcare program in partnership with the governments of Japan, Norway, and the Netherlands. Contact Us www.ifc.org/iqhealth ifc_healthcare@ifc.org Scan code below to join our community of practice, or visit http://bit.ly/3ZYt1PO
- 7. January February March April May June July August September October November December January February March April May June July August 19.2% 7.5% 10.2% 13% 8.9% 8.9% 7.9% 3.1% 3.4% 13.1% 4.9% 3.3% 1.4% 4.4% 6.4% 4.1% 0.7% 1.2% 0.4% 0.7% IMPLEMENTED FAST-TRACK CLINIC The number of emergency department cancellations in January 2022 resulted in a financial loss of about $5,000 per month. After implementing fast-track clinic operations, the losses prevented amounted to over $60,000 annually. In June 2022, the fast-track clinic served 634 patients. This number grew to 1,577 patients by October 2022. As of August 2023, 16% of emergency department patients were being served in fast-track clinics. DA R A L S H I FA H O S P I TA L , K U W A I T Dar Al Shifa Hospital (DASH) was established in 1963; it was the first private hospital built in Kuwait. The hospital provides inpatient facilities and emergency medical services across the region. In 2022, staff observed that patients left the emergency room without receiving care. What followed was an intensive quality improvement project focused on enhancing Emergency Department (ED) practices and patient flow. THE BUSINESS CASE: FAST-TRACKING EMERGENCY TRIAGE INCREASED PATIENTS SERVED THROUGH FAST-TRACK CLINIC BETTER EMERGENCY ROOM ACCESS BY INDEXING EMERGENCY SEVERITY DASH emergency department observed that 16% of patients triaged were Emergency Severity Index Levels 4 and 5, meaning the cases were less urgent and non-urgent. Fast-tracking these less-urgent and non- urgent cases led to shorter wait times and increased patient satisfaction. STAFF: 2,700+ BEDS: 249 PATIENT CANCELLATIONS DUE TO “CANNOT WAIT” FROM TOTAL CANCELLATIONS IN ADULT EMERGENCY DEPARTMENT COMPARED TO 5% DASH TARGET FINANCIAL RESULTS IMPACT OF INTERVENTION, IN US DOLLARS 2022 2023 16% CAN WAIT Redirected to fast-track clinic Level 5: Non-Urgent Condition Level 4: Less Urgent Condition 84% CAN NOT WAIT Level 3: Urgent Condition Level 2: Emergent Condition Level 1: Life-Threatening Condition -$5K MONTHLY LOSS OF REVENUE $60K LOSS OF REVENUE PREVENTED PER YEAR AFTER INTERVENTION BEFORE INTERVENTION 634 JUNE 2022 1,577 OCTOBER 2022 85% SATISFACTION ACHIEVED 2X SERVICE CAPACITY 5 MONTHS March 2024 Disclaimer: The figures and information depicted in this document were self-reported by the hospital named above and submitted during the “IFC Business Case for Healthcare Quality 2023” contest. SIZE: 34,972 m2 IMPROVED REFERRAL SYSTEM
- 8. What problem did the hospital face? In January 2022, we noticed a 19% increase in canceled invoices in the Emergency Department (ED). This resulted in an estimated financial loss of 5,000 USD per month. Because we are a private facility, anybody can walk in at any time. Patients come to the ED, check in, and receive an invoice followed by an appointment to be seen by a doctor. At some point in that process, patients began to leave the hospital. We discovered that our 20-minute wait to see a doctor was too long for most patients. How did the hospital alleviate the situation? We brought together the ED doctors, nurses, customer service, and IT staff from the Health Information department to hear from patients. Many of the ideas generated were simple but highly effective. For example, our patient’s top concern was having their feedback heard. So, we monitor it via an online platform called Press Ganey. When there were comments that required follow-up, our ED head called the patients directly to ask about their experiences and how we could improve. This had the greatest impact on return visits. We noticed that 20% of our patients were level 4 or 5 on the Emergency Severity Index (ESI), which meant they were less severe and did not need hospital resources. The question was how non-serious patients could bypass occupying an emergency bed, which added to wait time. Some of those patients needed sick leave notes. Others needed to be seen by a doctor because insurance demanded it, even if it was just a medication refill, lab, or routine checkup. Patients would even walk in for a copy of their medical report. So, we realized if we targeted this group differently, it could improve patient satisfaction and revenue. We decided to implement a fast-track clinic and educated patients and staff on the importance of using these services to reduce wait times. Can you talk more specifically about the steps taken to improve the situation? We assigned four additional nurses in the female section and three in the male section of the hospital during evening shifts. We installed screens in the waiting area to show each patient’s turn based on the queue number and triage level. We began using a color-coded process on ID bands that displayed the expected wait time. We changed the priority of lab tests to urgent if needed. We implemented a bedside payment process across the ED. Our ED charge nurse closely monitored patient discharge records via electronic medical records. Ultimately, we reduced the number of patients leaving without treatment within a month or two. Why does data make a difference? Data always provides insight into larger situations. For us, it was critical to identify patterns. In the case of the ED, we correlated the data to see which interventions would have the greatest impact on positive patient feedback, patient volume, and ED revenue. What challenges did the hospital face? We had a huge manpower shortage at this time, which made it difficult to effectively distribute staff across the hospital. One of the biggest obstacles was finding doctors who could be dedicated to staffing the fast-track clinic. These physicians do “We correlated the data to see which interventions would have the greatest impact on positive patient feedback” __________________ not see very critical cases, so for multiple reasons, there was less interest in staffing this function. So, we started with dedicated fast-track nurses. They were trained on patient intake, collecting and recording basic information, and were responsible for calling the doctor so that no time was wasted. Are there plans for the future? Yes. We have recently expanded our overall hospital with the addition of three new wings. This allows us to offer additional inpatient services. One of the closest areas to the emergency department was the laboratory. Due to the success of our fast-track clinic, the lab will be shifted out to create a full-fledged expansion of the Emergency Department. This expansion will actually double the emergency department capacity. We plan to have dedicated fast-track areas, areas for the Adult Emergency Department, Pediatrics, and Obstetrics. RESHAPING EMERGENCY CARE AMONG KUWAIT’S LARGEST HOSPITALS In an interview with IFC, Dar Al Shifa Hospital describes sweeping changes implemented after it observed almost 20 percent of patients leaving the Emergency Department without being treated. Jessy Jacob Quality Director Dar Al Shifa Hospital How Dar Al Shifa Hospital used data as its first line of defense in improving satisfaction, reputation, patient volume, and revenue. The IFC Business Case for Healthcare Quality contest is sponsored by IFC’s IQ-Healthcare program in partnership with the governments of Japan, Norway, and the Netherlands. Contact Us www.ifc.org/iqhealth ifc_healthcare@ifc.org Scan code below to join our community of practice, or visit http://bit.ly/3ZYt1PO