Neuroanatomía de Unión Craneocervical - Dr Ricardo Cázares Mejía
•Descargar como PPTX, PDF•
0 recomendaciones•6 vistas

Clase de curso Neuroanatomía Tumores cerebrales Abordaje Quirúrgico Neurocirujanos Neurocirugía Abordajes cerebrales Neurocirujano Neurooncología Neurocirugía Base de cráneo Neurocirugía columna cervical torácica lumbar Instituto Nacional de Neurología y Neurocirugía Microcirugía cerebral Neurocirugía endoscópica Dr. Ricardo Cázares Mejía Meningiomas Cirugía de columna vertebral

Recomendados
Recomendados
Más contenido relacionado
Más de RicardoCazaresMejia
Más de RicardoCazaresMejia (6)
Último
Último (20)
Neuroanatomía de Unión Craneocervical - Dr Ricardo Cázares Mejía
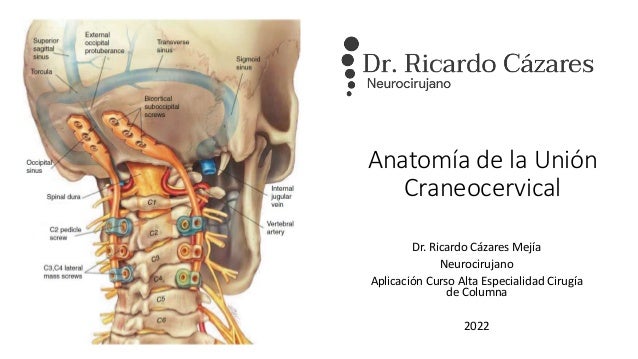
- 1. Anatomía de la Unión Craneocervical Dr. Ricardo Cázares Mejía Neurocirujano Aplicación Curso Alta Especialidad Cirugía de Columna 2022
- 2. CMN 20 de noviembre – Dr. Ricardo Cázares Mejía – Neurocirujano – www.doctorcazares.com
- 3. CMN 20 de noviembre – Dr. Ricardo Cázares Mejía – Neurocirujano – www.doctorcazares.com
- 4. CMN 20 de noviembre – Dr. Ricardo Cázares Mejía – Neurocirujano – www.doctorcazares.com
- 6. CMN 20 de noviembre – Dr. Ricardo Cázares Mejía – Neurocirujano – www.doctorcazares.com
- 7. CMN 20 de noviembre – Dr. Ricardo Cázares Mejía – Neurocirujano – www.doctorcazares.com
- 8. CMN 20 de noviembre – Dr. Ricardo Cázares Mejía – Neurocirujano – www.doctorcazares.com
- 9. CMN 20 de noviembre – Dr. Ricardo Cázares Mejía – Neurocirujano – www.doctorcazares.com
- 10. CMN 20 de noviembre – Dr. Ricardo Cázares Mejía – Neurocirujano – www.doctorcazares.com
- 11. Enfermedades Degenerativas Osificación LLP Espondilosis Cervical Multinivel Fusión Cervical Fallida Degeneración Segmento Adyacente Herniación Discal Trauma Síndrome medular central Dislocación fascetaria Fractura por estallamiento Espondiloptosis cervical Fracturas odontoideas Enfermedades Inflamatorias AR Occipitocervical Subluxación subaxial Espondilitis anquilosante Enfermedades Infecciosas Absceso epidural Osteomielitis Fusión Cervical Fallida Degeneración Segmento Adyacente Herniación Discal Miscelaneo Síndrome de Klippel Feil Siringomielia Desgarros durales Malformación de Chiari CMN 20 de noviembre – Dr. Ricardo Cázares Mejía – Neurocirujano – www.doctorcazares.com
- 12. CMN 20 de noviembre – Dr. Ricardo Cázares Mejía – Neurocirujano – www.doctorcazares.com
- 13. CMN 20 de noviembre – Dr. Ricardo Cázares Mejía – Neurocirujano – www.doctorcazares.com
- 15. Contacto Neurocirugia Cerebral Neurocirugía de Columna Vertebral E-mail: cazares@neuroquirurgicos.com Teléfono: 55 3585 0180 www.doctorcazares.com Consultorio: MediValle. Patricio Sanz 1307, Col. Del Valle Centro, Del. Benito Juárez. Consultorio: Star Médica Roma Torre II C-416. San Luis Potosí 143, Col. Roma Norte, Del. Cuauhtémoc. https://www.facebook.com/ricardo.cazares/ https://www.instagram.com/ricardocazaresmejia/ https://www.linkedin.com/in/ricardocazaresmejia/
Notas del editor
- T1 sagittal (a, b, c, d, and e) and coronal MR images (f). Chamberlain’s line (a), McGregor’s line (b), Wackenheim’s clivus baseline (c), basal angle (d), clivus-canal angle (e), and atlanto-occipital joint angle (f)
- Lateral x-ray shows a normal alignment of the cervical spine. On most occasions, cervical lordosis occurs at the C1–2 segment. (A) C0–1 segment is kyphotic, and the C1 slope is posteriorly slanted. (B) C0–2 segment is a hyperlordotic, and the C1 slope is reversely slanted to maintain the patient’s horizontal gaze with sagittal malalignment and subaxial cervical kyphotic deformity patient. (C) Craniovertebral junction kyphotic deformity patient shows a hyperlordotic compensation in the subaxial cervical spine and negative sagittal imbalance to maintain gaze.
- transoral surgical route, lateral mass screw xations, transarticular screw xations, occipitocervical fusions, and lateral approaches to anterior foramen magnum lesions has made learning of the anatomy of the bony–vascular relationship in the CVJ more relevant. I
- Safe screw implantation is from the middle of the posterior surface of the inferior facet of the atlas, directed 15° on the medial to sagittal plane and 15° on the superior to axial plane. If the screw is implanted from the superior and medial third of a screwable pedicle, and the trajectory of the screw is 40° on the medial to sagittal plane and 20° on the superior to axial plane, the probability of entering into the vertebral artery foramen is almost nil.
- (A, B) Sagittal T2 magnetic resonance imaging (MRI) and sagittal reconstruction computed tomography (CT) image showing odontoid compression over the brain stem and upper cervical cord. Odontoid tip (white arrow) is located above the foramen magnum. (C) Parasagittal reconstruction CT scan showing C1–2 facet subluxation and severe joint mutilation of the C0–1 facet joint (arrow). (D) Postoperative x-ray showing the final construct of C0–2 instrumentation. (E, F) Postoperative sagittal T2 MRI and sagittal reconstruction CT image showing early reduction of retroodontoid rheumatoid pannus (white arrow) and odontoid tip (black arrow) is pulled down below the foramen magnum. (G) Parasagittal reconstruction CT scan shows vertical distraction and intra-articular fusion (white arrow) inside the C1–2 facet joints.