ASMA VS CRISIS
ASMÁTICA
FACTORESDE
RIESGO
CLASIFICACIÓN
DE LA CRISIS
ASMÁTICA
CUADRO
CLÍNICO
01
02
04
05
TABLE OF CONTENTS
03
FISIOPATOLOGÍ
A
DIAGNÓSTICO
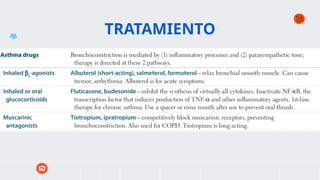
TRATAMIENTO
06
07
3.
01
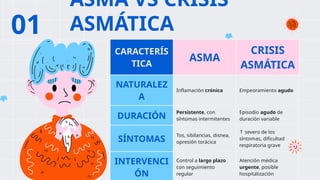
ASMA VS CRISIS
ASMÁTICA
CARACTERÍS
TICA
ASMA
CRISIS
ASMÁTICA
NATURALEZ
A
Inflamacióncrónica Empeoramiento agudo
DURACIÓN
Persistente, con
síntomas intermitentes
Episodio agudo de
duración variable
SÍNTOMAS
Tos, sibilancias, disnea,
opresión torácica
↑ severo de los
síntomas, dificultad
respiratoria grave
INTERVENCI
ÓN
Control a largo plazo
con seguimiento
regular
Atención médica
urgente, posible
hospitalización
4.
FACTORES DE RIESGO
●Exposición a alérgenos (polvo, ácaros, polen)
● Antecedentes familiares (OR) de 2.957 y 3.051
● Infecciones respiratorias virales
● Exposición al humo de tabaco
● Nacimiento por cesárea (OR = 3.316)
● Uso de mentolados (OR = 4.846)
● Obesidad (OR = 3.116)
● IPA positivo
CRITERIOS MAYORES CRITERIOS MENORES
Padres con asma Sibilancias no asociadas a
resfriados
Eccema atópico Eosinofilia 4%
≥
Sensibilización a algún
alergeno
Alergia al huevo, leche,
frutos secos
Rinitis alérgica
5.
FISIOPATOLOGÍA - Infecciones
respiratoriasvirales
- Exposición a alérgenos
- Contaminantes
ambientales
- Ejercicio físico intenso
- Estrés emocional
DESENCADEN
ANTES
BRONCOCONSTRIC
CIÓN
INFLAMACIÓN
AGUDA
HIPERSECRECIÓN
DE MOCO
ALTERACIÓN DEL
INTERCAMBIO
GASEOSO
6.
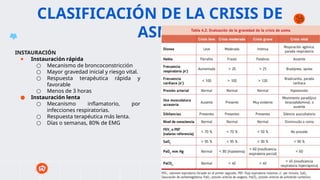
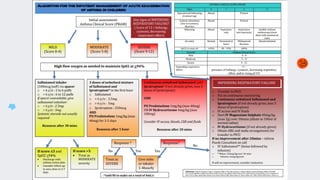
CLASIFICACIÓN DE LACRISIS DE
ASMA
INSTAURACIÓN
● Instauración rápida
○ Mecanismo de broncoconstricción
○ Mayor gravedad inicial y riesgo vital.
○ Respuesta terapéutica rápida y
favorable
○ Menos de 3 horas
● Instauración lenta
○ Mecanismo inflamatorio, por
infecciones respiratorias.
○ Respuesta terapéutica más lenta.
○ Días o semanas, 80% de EMG
7.
CUADRO CLÍNICO
● Incrementode sintomas
● Incrementos de tos,
especialmente nocturna.
● Letargia
● Respuesta pobre a
medicamentos.
● Disnea
8.
DIAGNÓSTICO
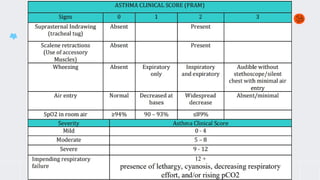
PULMONARY SCORE PARALA VALORACIÓN CLÍNICA DE LA CRISIS DE ASMA EN NIÑOS
Puntuación Frecuencia respiratoria
<6 años >6 años
Sibilancias Uso de ECM
0 <30 <20 No No
1 31-45 21-35 Final de la espiración Incremento
2 46-60 36-50 Toda la espiración (estetoscopio) Aumentado
3 >60 >50 Inspiración y espiración sin estetoscopio Actividad máxima
PULMONARY SCORE SAT O2
LEVE 0 - 3 >94%
MODERADA 4 - 6 91-94%
GRAVE 7 - 9 <91%
En caso de discordancia se usa el
parámetro de mayor gravedad
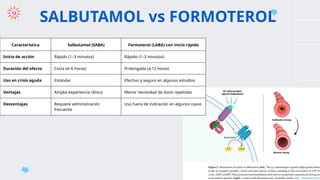
SALBUTAMOL vs FORMOTEROL
CaracterísticaSalbutamol (SABA) Formoterol (LABA) con inicio rápido
Inicio de acción Rápido (1–3 minutos) Rápido (1–3 minutos)
Duración del efecto Corta (4–6 horas) Prolongada ( 12 horas)
≥
Uso en crisis aguda Estándar Efectivo y seguro en algunos estudios
Ventajas Amplia experiencia clínica Menor necesidad de dosis repetidas
Desventajas Requiere administración
frecuente
Uso fuera de indicación en algunos casos
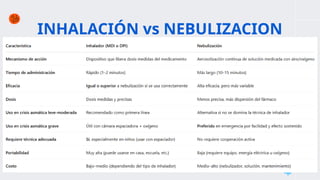
INHALACIÓN vs NEBULIZACION
MERCURY
Mercuryis the smallest
planet of them all
MARS
Despite being red, Mars
is actually a cold planet
VENUS
Venus is the second
planet from the Sun
SATURN
Saturn is composed of
hydrogen and helium
JUPITER
Jupiter is the biggest
planet of them all
NEPTUNE
Neptune is the farthest
planet from the Sun
22.
● Global Initiativefor Asthma. Global Strategy for Asthma Management and Prevention, 2024.
Available from: https://ginasthma.org/2024-report/
● Reyes Flores C, Martínez Vergara A. Crisis asmática. In: Medicina de Urgencias. 1ª ed. Buenos
Aires: Editorial Médica Panamericana; 2022. p. 193-200.
● GEMA 5.4. Guía Española para el Manejo del Asma. 2024. Disponible en:
https://www.separ.es/node/2045
● Velazco L. Asociación de la severidad de crisis asmática y obesidad en pacientes pediátricos,
área de emergencia de pediatría del Hospital Ramiro Prialé Prialé, periodo enero a diciembre
2022. Universidad Nacional del Centro del Perú; 2024. Disponible en:
https://repositorio.uncp.edu.pe/handle/20.500.12894/11374
● Instituto Nacional de Salud del Niño – San Borja. Guía de Práctica Clínica para el Diagnóstico y
Tratamiento de Asma en Pediatría. Lima: INSN-SB; 2023. Disponible en:
https://portal.insnsb.gob.pe/docs-trans/resoluciones/archivopdf.php?pdf=2024%2FGPC+Asma
+2023+4+1F.pdf
● Hospital de Emergencias Villa El Salvador. Lima: Guía de Práctica Clínica para el Diagnóstico y
tratamiento de Crisis de Asma en Paciente Pediátrico del Hospital De Emergencia Villa El
Salvador. 2023
REFERENCIAS BIBLIOGRÁFICAS
23.
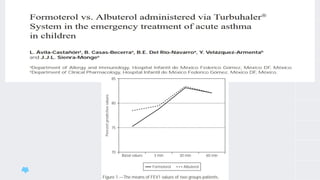
● Ávila-Castañón, L.,Casas-Becerra, B., Del Río-Navarro, B. E., Velázquez-Armenta, Y., & Sienra-
Monge, J. J. L. (2004). Formoterol vs. Albuterol administered via Turbuhaler® System in the
emergency treatment of acute asthma in children. Allergologia et Immunopathologia, 32(1),
18–20. doi:10.1016/s0301-0546(04)79218-6
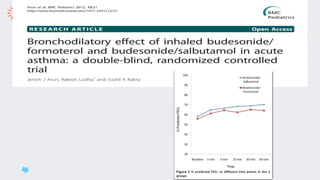
● Bronchodilatory effect of inhaled budesonide/formoterol and budesonide/salbutamol in acute
asthma: a double-blind, randomized controlled trial | BMC Pediatrics | Full Text [Internet]. .
Disponible en:
https://bmcpediatr.biomedcentral.com/articles/10.1186/1471-2431-12-21?utm_source=chatgpt
.com
● Bateman E, Fairall L, Lombardi D, English R. Budesonide/formoterol and formoterol provide
similar rapid relief in patients with acute asthma showing refractoriness to salbutamol.
Respiratory Research. 24 de enero de 2006;7(1):13.
● Hatter L, Bruce P, Braithwaite I, Holliday M, Fingleton J, Weatherall M, et al. ICS-formoterol
reliever versus ICS and short-acting β2-agonist reliever in asthma: a systematic review and
meta-analysis. ERJ Open Res. 25 de enero de 2021;7(1):00701-2020.
REFERENCIAS BIBLIOGRÁFICAS
24.
● Cates CJ,Welsh EJ, Rowe BH. Holding chambers (spacers) versus nebulisers for beta-
agonist treatment of acute asthma. Cochrane Database Syst Rev. 2013;(9):CD000052.
Disponible en:
https://www.cochrane.org/CD000052/AIRWAYS_holding-chambers-spacers-versus-n
ebulisers-for-delivery-of-beta-agonist-relievers-in-the-treatment-of-an-asthma-attac
k
● MR, Sellers AR, Darville KK, Teppa-Sanchez B, McKinley SD, Martin M, Goldenberg
NA, Nakagawa TA, Sochet AA. Dexamethasone versus methylprednisolone for critical
asthma: A single center, open-label, parallel-group clinical trial. Pediatr Pulmonol.
2023 Jun;58(6):1719-1727. doi: 10.1002/ppul.26386. Epub 2023 Mar 17. PMID:
36929864.
REFERENCIAS BIBLIOGRÁFICAS
25.
CREDITS: This presentationtemplate was created by Slidesgo,
including icons by Flaticon and infographics & images by
Freepik
THANKS
Notas del editor
#15 The review suggests that high-dose formoterol, administered via DPI, is well tolerated and provides similar rapid and effective bronchodilation as high- and repetitive-dose salbutamol or terbutaline, administered via metered-dose inhaler or nebulizer, in the treatment of acute asthma. The fact that formoterol required less repeated rescue medication to balance it is probably the cost difference. Therefore, formoterol could replace conventional SABAs as reliever medication in the acute care setting. Future trials are needed to assess the comparison of formoterol with SABAs in patients with acute life-threatening asthma and to examine the use of formoterol plus inhaled corticosteroids in acute asthma treatment.
#16 At screening (t = -20 minutes), salbutamol 400 µg was administered to all patients to establish their relative refractoriness to β2-agonist therapy. Patients in the formoterol group received formoterol 9 µg, 2 inhalations at t = -5 minutes and 2 inhalations at 0 minutes (total dose 36 µg). Patients treated with budesonide/formoterol received budesonide/formoterol 320/9 µg, 2 inhalations at t = -5 minutes and 2 inhalations at 0 minutes (total dose 1280/36 µg). The timing of study drug administration is shown by vertical dotted lines on the figure. Patients received oral prednisolone 60 mg 90 minutes after the last administration of study drug.






![● Ávila-Castañón, L., Casas-Becerra, B., Del Río-Navarro, B. E., Velázquez-Armenta, Y., & Sienra-
Monge, J. J. L. (2004). Formoterol vs. Albuterol administered via Turbuhaler® System in the
emergency treatment of acute asthma in children. Allergologia et Immunopathologia, 32(1),
18–20. doi:10.1016/s0301-0546(04)79218-6
● Bronchodilatory effect of inhaled budesonide/formoterol and budesonide/salbutamol in acute
asthma: a double-blind, randomized controlled trial | BMC Pediatrics | Full Text [Internet]. .
Disponible en:
https://bmcpediatr.biomedcentral.com/articles/10.1186/1471-2431-12-21?utm_source=chatgpt
.com
● Bateman E, Fairall L, Lombardi D, English R. Budesonide/formoterol and formoterol provide
similar rapid relief in patients with acute asthma showing refractoriness to salbutamol.
Respiratory Research. 24 de enero de 2006;7(1):13.
● Hatter L, Bruce P, Braithwaite I, Holliday M, Fingleton J, Weatherall M, et al. ICS-formoterol
reliever versus ICS and short-acting β2-agonist reliever in asthma: a systematic review and
meta-analysis. ERJ Open Res. 25 de enero de 2021;7(1):00701-2020.
REFERENCIAS BIBLIOGRÁFICAS](https://image.slidesharecdn.com/crisisasmtica-1-250527105239-23752dc0/85/CRISIS-ASMATICA-EN-PEDIATRIA-2025-23-320.jpg)