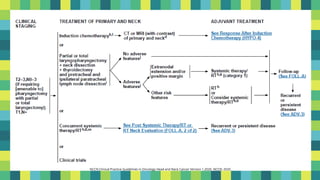
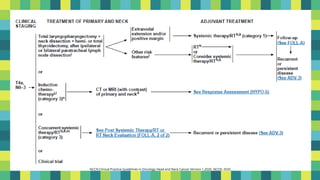
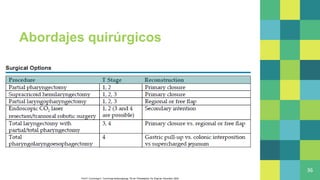
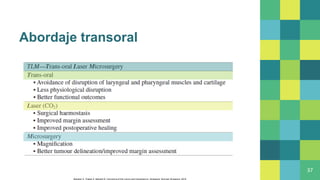
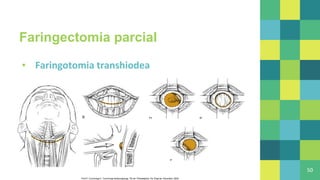
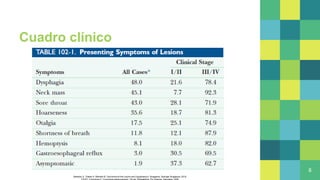
Este documento describe la anatomía, epidemiología, presentación clínica, diagnóstico, patología, estadificación y tratamiento de las neoplasias de hipofaringe. Las neoplasias de hipofaringe generalmente son carcinoma de células escamosas y se presentan con disfagia, masa en cuello u otros síntomas. Se diagnostican mediante TAC, RM u otros estudios de imagen y se estadifican usando el sistema TNM. Los tratamientos incluyen cirugía como faringectomía parcial o abordajes transorales




![Imagen
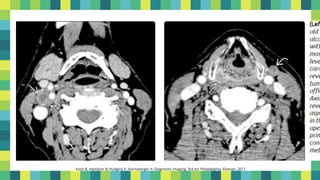
▪ Evaluación pretratamiento
10
TAC
• (invasión cartílago
precisión general 75%
[S, E 84%])
RM
• (invasión cartílago
precisión general 78%
[S: 89-100%, E: 62%])](https://image.slidesharecdn.com/hipofaringeneoplasiasmalignas-211025150257/85/Hipofaringe-neoplasias-malignas-10-320.jpg)