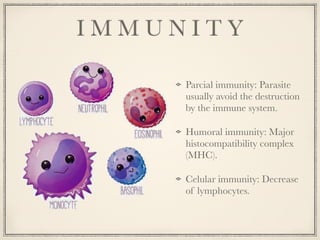
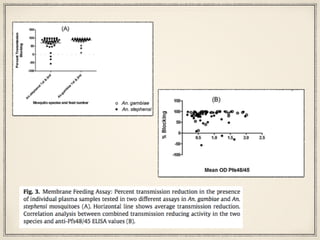
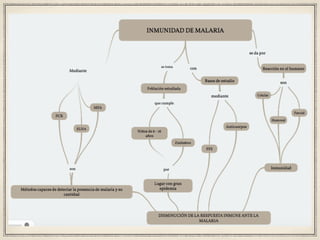
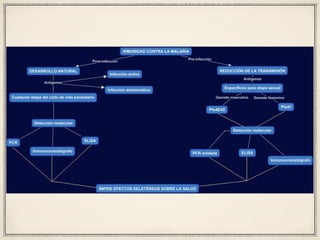
El estudio investiga la inmunidad parcial al parásito de la malaria en niños de 6 a 16 años en Zimbabwe, expuestos a bajos niveles de transmisión. A pesar de la exposición, el desarrollo de una inmunidad protectora real parece poco probable, lo que sugiere que la resistencia se logra solo con repetidas exposiciones. Se plantea la posibilidad de que el desarrollo de una resistencia en la población facilite la creación de una vacuna en el futuro.