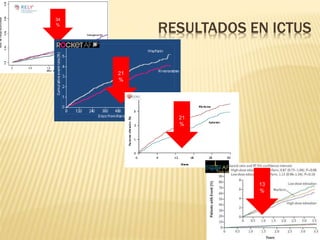
El documento aborda la relación entre la fibrilación auricular (FA) y el riesgo de accidente cerebrovascular (ictus) y mortalidad, destacando factores de riesgo en pacientes con FA no valvular. Se presenta la escala CHA2DS2-VASc para evaluar el riesgo de ictus, donde los pacientes son anticoagulados en un 50%. Además, se menciona la necesidad de mejorar la gestión y el manejo de la FA en la atención primaria.




![(a) Factores de riesgo de ictus y tromboembolismo en la FA no valvular
Factores de riesgo mayores
Factores de riesgo menos validados o con menos
poder
Antecedentes de ictus, AIT o embolismo sistémico
Edad ≥ 75 años
Insuficiencia cardíaca o disfunción sistólica del
ventrículo izquierdo de moderada a severa (p. ej. FE VI
≤ 40%)
Hipertensión-diabetes mellitus
Sexo femenino-edad: 657-74 años
Enfermedad vasculara
(b) Escala de riesgo de ictus en FA: CHa2DS2-VASc [Congestive heart failure, Hypertension, Age ≥ 75 (2 =
doubled), Diabetes Stroke (2 = doubled), Vascular disease, Age 65-74, Sex Category (female)]
(Nota: la máxima puntuación es 9, ya que la edad puede aportar 0, 1 o 2 puntos)
Factor de riesgo Puntuación
Insuficiencia cardíaca congestiva/disfunción VI 1
Hipertensión 1
Edad ≥ 75 años 2
Diabetes mellitus 1
Ictus/AIT/tromboembolismo 2
Enfermedad vasculara 1
Edad: 65-74 años 1
Sexo femenino 1
Puntuación máxima 9
Lip GY, et al. Stroke. 2010;41:2731-8.
Camm AJ, et al. Guidelines for the management of atrial fibrillation: The Task Force for the Management of AF of the ESC. Eur Heart J 2010;doi:10.1093/eurheartj/ehq278.
1.30%
2.20%
3.20%
4.00%
6.70%
9.80% 9.60%
6.70%
15.20%
0.00%
2.00%
4.00%
6.00%
8.00%
10.00%
12.00%
14.00%
16.00%
1 2 3 4 5 6 7 8 9
EVALUACIÓN DE RIESGO ICTUS](https://image.slidesharecdn.com/presentacinnacos-140715043812-phpapp01/85/Presentacion-nac-os-6-320.jpg)