Descargado 11 veces



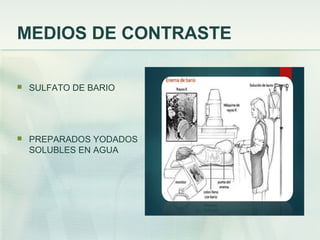






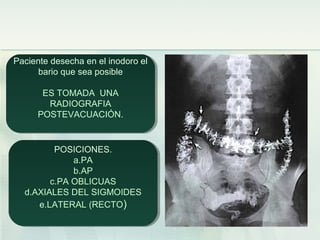


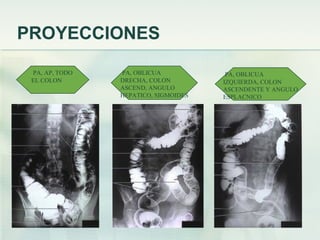
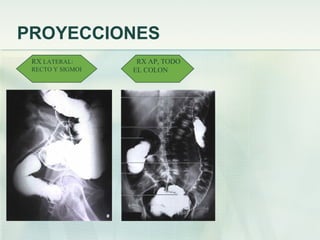






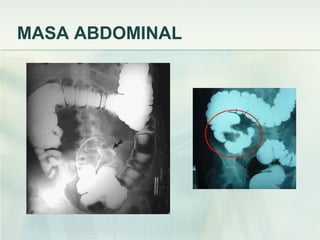

Este documento proporciona información sobre el enema baritado, un procedimiento radiológico para visualizar el colon mediante la administración de un medio de contraste. Explica que el enema baritado permite evaluar trastornos del colon como la enfermedad de Crohn, diverticulitis y cáncer de colon. Describe el procedimiento, incluida la preparación del paciente, las proyecciones radiográficas y los posibles hallazgos como masas abdominales o complicaciones como perforaciones.



































































