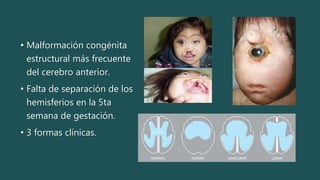
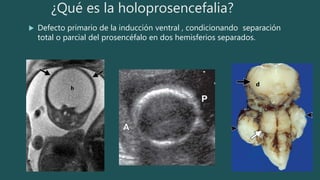
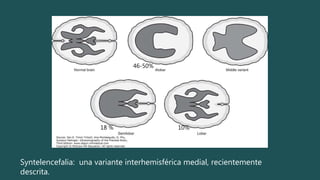
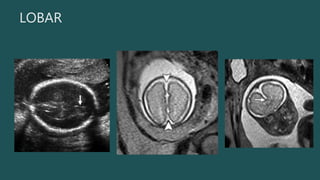
La holoprosencefalia es una malformación congénita del cerebro anterior donde falta la separación de los hemisferios cerebrales. Existen tres formas clínicas: alobar, semilobar y lobar. La etiología incluye anomalías cromosómicas, mutaciones genéticas y teratógenos. El diagnóstico prenatal se puede establecer desde la semana 6 y se basa en anomalías faciales y la ausencia del cavum septum pellucidum. El pronóstico depende de la severidad de las malformaciones cerebrales y facial

















































![Morfología_de_las_malformaciones[1].pdf](https://cdn.slidesharecdn.com/ss_thumbnails/morfologiadelasmalformaciones1-250915030152-f3a9eddd-thumbnail.jpg?width=640&height=640&fit=bounds)
















