3. Ibanez B, James S, Agewall S, Antunes MJ, Bucciarelli-Ducci C, Bueno H, et al. 2017 ESC Guidelines for the management of acute myocardial infarction in
patients presenting with ST-segment elevation. Eur Heart J. 2018;39(2):119–77.
4. Manejo
Ibanez B, James S, Agewall S, Antunes MJ, Bucciarelli-Ducci C, Bueno H, et al. 2017 ESC Guidelines for the management of acute myocardial infarction in
patients presenting with ST-segment elevation. Eur Heart J. 2018;39(2):119–77.
TIEMPO ES
MIOCARDIO
5. Monitorización
• Arritmias letales
Ibanez B, James S, Agewall S, Antunes MJ, Bucciarelli-Ducci C, Bueno H, et al. 2017 ESC Guidelines for the management of acute myocardial infarction in
patients presenting with ST-segment elevation. Eur Heart J. 2018;39(2):119–77.
6. Alivio del dolor y sensación de falta de aire
• Dolor
• Morfina retrasa la absorción del clopidogrel
(p=0.025), el inicio de tiempo de acción (p<0-01) y el
efecto (AUC -34% p=0.001)
• Derivados de opiáceos
• Dosis: 2 – 4 mg IV c/15 min
• Ticagrelor menor absorción, menor concentración
(p<0.05)
• Oxigeno
• Indicado en pacientes con hipoxemia (Sao2 menor
de 90% o PaO2 menor de 60 mmhg)
• Distrés respiratorio (FR>25 / SaO2 <90%
• VNI (CPAP / BIPAP) vs terapia respiratoria de alto flujo
• META SaO2 95%
• VMI
Ibanez B, James S, Agewall S, Antunes MJ, Bucciarelli-Ducci C, Bueno H, et al. 2017 ESC Guidelines for the management of acute myocardial infarction in
patients presenting with ST-segment elevation. Eur Heart J. 2018;39(2):119–77.
8. Tratamiento de reperfusión: Antiagregantes plaquetarios
Tratamiento de reperfusión
Fibrinolisis Angioplastia Primaria
AAS 150 a 300 mg masticable
Dosis de mantenimiento: 75 a 100 mg VO c/ 24 hrs
Clopidogrel < 75 años: 300 mg vo
> 75 años: 75 mg vo
600 mg VO
Dosis de mantenimiento: 75 mg VO cada 24 hrs
Prasugrel No recomendado 60 mg
Dosis de mantenimiento: 10 mg VO cada 24 hrs
Ticagrelor No recomendado 180 mg
Dosis de mantenimiento: 90 mg VO cada 12 hrs
Ibanez B, James S, Agewall S, Antunes MJ, Bucciarelli-Ducci C, Bueno H, et al. 2017 ESC Guidelines for the management of acute myocardial infarction in
patients presenting with ST-segment elevation. Eur Heart J. 2018;39(2):119–77.
9. Ibanez B, James S, Agewall S, Antunes MJ, Bucciarelli-Ducci C, Bueno H, et al. 2017 ESC Guidelines for the management of acute myocardial infarction in
patients presenting with ST-segment elevation. Eur Heart J. 2018;39(2):119–77.
10. • Mecanismo de acción: El
clopidogrel inhibe selectivamente el
receptor P2Y12, que es uno de los
receptores plaquetarios de ADP.
• Antagoniza la inhibición inducida
por el ADP, que resulta en un
incremento de
adenosinmonofosfato cíclico (AMPc)
• Inhibe la unión del receptor
GpIIb/IIIa al fibrinógeno
Clopidogrel
Inhibidores de la P2Y2
Ibanez B, James S, Agewall S, Antunes MJ, Bucciarelli-Ducci C, Bueno H, et al. 2017 ESC Guidelines for the management of acute myocardial infarction in
patients presenting with ST-segment elevation. Eur Heart J. 2018;39(2):119–77.
11. Prasugrel
• Mecanismo de acción:
El prasugrel requiere dos
pasos metabólicos para
formar su metabolito activo,
que es químicamente
parecido al metabolito activo
del clopidogrel.
Inhibidores de la P2Y2 IAMSEST
Ibanez B, James S, Agewall S, Antunes MJ, Bucciarelli-Ducci C, Bueno H, et al. 2017 ESC Guidelines for the management of acute myocardial infarction in
patients presenting with ST-segment elevation. Eur Heart J. 2018;39(2):119–77.
12. • Pertenece a una nueva clase
química, las
ciclopentiltriazolopirimidinas,
y es un inhibidor oral que se
une de forma reversible
al P2Y12 con una vida media
plasmatica de ~12 h.
Ticagrelor
Inhibidores de la P2Y2 IAMSEST
Ibanez B, James S, Agewall S, Antunes MJ, Bucciarelli-Ducci C, Bueno H, et al. 2017 ESC Guidelines for the management of acute myocardial infarction in
patients presenting with ST-segment elevation. Eur Heart J. 2018;39(2):119–77.
13. Clopidogrel Prasugrel Ticagrelor
Clase Tienopiridina Tienopiridina Triazolopirimidina
Reversibilidad Irreversible Irreversible Reversible
Activación Profarmaco , limitado por
metabolización
Profarmaco , limitado por
metabolización
Fármaco activo
Inicio del efecto* 2 – 4 hrs 30 min 30 min
Duración del efecto 3 – 10 días 5 – 10 días 3 – 4 días
Interrupción antes de la Qx
mayor
5 días 7 días 5 días
Inhibidores de la P2Y2 IAMSEST
Ibanez B, James S, Agewall S, Antunes MJ, Bucciarelli-Ducci C, Bueno H, et al. 2017 ESC Guidelines for the management of acute myocardial infarction in
patients presenting with ST-segment elevation. Eur Heart J. 2018;39(2):119–77.
14. • ASA (Lo más pronto posible!!!)
• INHIBIDORES DE LA 2PY12
• Se prefiere Prasugrel o Ticagrelor, estos
fármacos tienen un inicio de acción más
rápido, mayor potencia y mejores resultados
clínicos que el clopidogrel)
• Prasugrel
• CONTRAINDICADO EN EVC O AIT PREVIO,
ENFERMEDAD HEPATICA MODERADA O
GRAVE
• NO RECOMENDADO EN <60 KG O >75 AÑOS
• Clopidogrel
• Único utilizado para trombólisis
• Si no se dispone de los anteriores(o estén
contraindicados), en su lugar se puede
emplear clopidogrel 600 mg vía oral
Ibanez B, James S, Agewall S, Antunes MJ, Bucciarelli-Ducci C, Bueno H, et al. 2017 ESC Guidelines for the management of acute myocardial infarction in
patients presenting with ST-segment elevation. Eur Heart J. 2018;39(2):119–77.
Antiagregantes plaquetarios
15. Estudios
• CLARITY TIMI 28
• CLOPIDOGREL
• TIMI TRITON 38
• PRASUGREL EFICACIA 60 MG DE CARGA Y 10 DE MANTENIMIENTO DIARIO
• PLATO
• TICAGRELOR DOSIS DE CARGA 180 MG Y 90 MG DE MANTENIMIENTO
Ibanez B, James S, Agewall S, Antunes MJ, Bucciarelli-Ducci C, Bueno H, et al. 2017 ESC Guidelines for the management of acute myocardial infarction in
patients presenting with ST-segment elevation. Eur Heart J. 2018;39(2):119–77.
16. Tratamiento de reperfusión
Fibrinolisis Angioplastia Primaria
HNF 60 U/kg IV (máx 4000U)
120 U/kg/h infusión
(máx 1000 U/hra)
70 U/kg IV
Enoxaparina < 75 años 30 mg IV
después 1 mg/ kg SC c/12 hrs
> 75 años 0.75 mg c/12 hrs SC
TFG <30ml/min 1mg/kg c/24 hrs SC
0.5 mg/kg/ IV
Fondaparinux 2.5 mg IV posteriormente
2.5 mg SC c/24 hrs
No se recomienda
Bivalirudina No recomendado 0.75 mg/kg IV en infusión
1.75 mg/kg/hra hasta 4 hrs
post PCI
Ibanez B, James S, Agewall S, Antunes MJ, Bucciarelli-Ducci C, Bueno H, et al. 2017 ESC Guidelines for the management of acute myocardial infarction in
patients presenting with ST-segment elevation. Eur Heart J. 2018;39(2):119–77.
Tratamiento de reperfusión: Anticoagulantes
17. • Inhibidores indirectos de la trombina
• HNF; heparinas de bajo peso molecular (HBPM).
• Inhibidores indirectos del factor Xa
• Fondaparinux.
Inhibidores indirectos de la coagulación
(requieren antitrombina para una acción
completa).
• Inhibidores directos del factor Xa
• Apixabán, rivaroxabán, otamixabán.
• Inhibidores directos de la trombina
• Bivalirudina, dabigatrán
Inhibidores directos de la coagulación
Ibanez B, James S, Agewall S, Antunes MJ, Bucciarelli-Ducci C, Bueno H, et al. 2017 ESC Guidelines for the management of acute myocardial infarction in
patients presenting with ST-segment elevation. Eur Heart J. 2018;39(2):119–77.
18. Ibanez B, James S, Agewall S, Antunes MJ, Bucciarelli-Ducci C, Bueno H, et al. 2017 ESC Guidelines for the management of acute myocardial infarction in
patients presenting with ST-segment elevation. Eur Heart J. 2018;39(2):119–77.
19. • Heparina de bajo peso molecular
• La HBPM tiene una relación dosis-efecto más
predecible que la HNF y menos riesgo de
trombocitopenia.
• El fármaco más utilizado en los SCA es la
enoxaparina .
Inhibidores indirectos de la coagulación
(requieren antitrombina para una acción
completa).
Ibanez B, James S, Agewall S, Antunes MJ, Bucciarelli-Ducci C, Bueno H, et al. 2017 ESC Guidelines for the management of acute myocardial infarction in
patients presenting with ST-segment elevation. Eur Heart J. 2018;39(2):119–77.
20. • Inhibidores indirectos de la trombina
• Heparina no fraccionada
• La HNF tiene un perfil farmacocinético con gran variabilidad
interindividual y una ventana terapéutica estrecha. Se
recomienda la administración
Inhibidores indirectos de la coagulación
Ibanez B, James S, Agewall S, Antunes MJ, Bucciarelli-Ducci C, Bueno H, et al. 2017 ESC Guidelines for the management of acute myocardial infarction in
patients presenting with ST-segment elevation. Eur Heart J. 2018;39(2):119–77.
21. • Inhibidores directos de la trombina
• Bivalirudina
• La bivalirudina se une directamente a la trombina e inhibe
la conversión inducida por la trombina de fibrinógeno a
fibrina. Inactiva la trombina unida a fibrina y la trombina
libre
• La bivalirudina se elimina por vía renal y tiene una vida
media de 25 min tras el cese de la infusión
Inhibidores directos de la coagulación
Ibanez B, James S, Agewall S, Antunes MJ, Bucciarelli-Ducci C, Bueno H, et al. 2017 ESC Guidelines for the management of acute myocardial infarction in
patients presenting with ST-segment elevation. Eur Heart J. 2018;39(2):119–77.
22. Ibanez B, James S, Agewall S, Antunes MJ, Bucciarelli-Ducci C, Bueno H, et al. 2017 ESC Guidelines for the management of acute myocardial infarction in
patients presenting with ST-segment elevation. Eur Heart J. 2018;39(2):119–77.
23. • Heparina no fraccionada
• La dosis debe seguir las recomendaciones
estándar para la ICP (es decir, un bolo
inicial de 70-100 U/kg)
• No hay datos solidos que recomienden
utilizar el tiempo de coagulación activado
para establecer la dosis o monitorizar la
HNF, pero si se emplea, no debe retrasar
la recanalización de la ARI.
Ibanez B, James S, Agewall S, Antunes MJ, Bucciarelli-Ducci C, Bueno H, et al. 2017 ESC Guidelines for the management of acute myocardial infarction in
patients presenting with ST-segment elevation. Eur Heart J. 2018;39(2):119–77.
Anticoagulantes
Las opciones de anticoagulación para la ICP
primaria incluyen HNF, enoxaparina y
bivalirudina.
24. Estudios
• OASIS 6
• ATOLL LA ENOXAPARINA VS HNF LOS PACIENTES TIENE UNA
ADECUADA EVOLUCION
• EXTRACT TIMI 25 SE ADMINISTRO ENOXAPARINA A PACIENTES CON
MENOS DE 75 AÑOS O UNA TFG <30ML/KG
Ibanez B, James S, Agewall S, Antunes MJ, Bucciarelli-Ducci C, Bueno H, et al. 2017 ESC Guidelines for the management of acute myocardial infarction in
patients presenting with ST-segment elevation. Eur Heart J. 2018;39(2):119–77.
25. Tx
de reperfusión
Estatinas
• Varios estudios clínicos han establecido
el beneficio de iniciar precozmente un
tratamiento intensivo con estatinas de
los pacientes con SCA
• Recomendable empezar terapia con
• estatinas de alta intensidad lo más
temprano posible, a menos que este
contraindicado y mantener a largo plazo
• Atorvastatina 80 mg
• Intolerancia : Ezetimiba (IMPROVE – IT)
Beneficios
en
resultados
de ICP
Beneficio
en tamaño
IM (SPECT)
Beneficio
en eventos
a largo
plazo
Ibanez B, James S, Agewall S, Antunes MJ, Bucciarelli-Ducci C, Bueno H, et al. 2017 ESC Guidelines for the management of acute myocardial infarction in
patients presenting with ST-segment elevation. Eur Heart J. 2018;39(2):119–77.
26. Estudios
• Miracle APARTE DE REDUCIR COLESTEROL, LDL, DISMINUYE LOS
EVENTOS ISQUEMICOS RECURRENTES ASI COMO PLEIOTROPICOS
Ibanez B, James S, Agewall S, Antunes MJ, Bucciarelli-Ducci C, Bueno H, et al. 2017 ESC Guidelines for the management of acute myocardial infarction in
patients presenting with ST-segment elevation. Eur Heart J. 2018;39(2):119–77.
28. IECA y ARA II
• Una revisión sistemática de los estudios que administraron
precozmente IECA a pacientes con IAMCEST ha indicado que este
tratamiento es seguro, se tolera bien y se asocia con una reducción
pequeña pero significativa de la mortalidad a los 30 días
• Captopril 12.5 mg VO
• Valsartan 20 mg VO
30. REPERFUSIÓN
Ibanez B, James S, Agewall S, Antunes MJ, Bucciarelli-Ducci C, Bueno H, et al. 2017 ESC Guidelines for the management of acute myocardial infarction in
patients presenting with ST-segment elevation. Eur Heart J. 2018;39(2):119–77.
31. ICP VS FIBRINOLISIS PAMI TRIAL
Ibanez B, James S, Agewall S, Antunes MJ, Bucciarelli-Ducci C, Bueno H, et al. 2017 ESC Guidelines for the management of acute myocardial infarction in
patients presenting with ST-segment elevation. Eur Heart J. 2018;39(2):119–77.
33. FIBRINOLISIS INDICACIONES
• PREVIENE 30 MUERTES DE CADA 1000 PACIENTES
• EL MAYOR BENEFICIO DENTRO DE LAS PRIMERAS 3 HRS
• CONSIDERAR LOS POSIBLES DAÑOS (CONTRAINDICACIONES)
• USO PRE HOSPITALARIO REDUCE 17% LA MORTALIDAD TEMPRANA
Ibanez B, James S, Agewall S, Antunes MJ, Bucciarelli-Ducci C, Bueno H, et al. 2017 ESC Guidelines for the management of acute myocardial infarction in
patients presenting with ST-segment elevation. Eur Heart J. 2018;39(2):119–77.
34. FIBRINOLISIS DOSIS
Ibanez B, James S, Agewall S, Antunes MJ, Bucciarelli-Ducci C, Bueno H, et al. 2017 ESC Guidelines for the management of acute myocardial infarction in
patients presenting with ST-segment elevation. Eur Heart J. 2018;39(2):119–77.
• ESTREPTOCINASA
GUSTO
• ALTEPLASE vs TNK
ASSENT los dos son
iguales ninguno
disminuye la
mortalidad, pero los
sangrados menores
les fue mejor con tnk,
mas fácil de aplicar
35. FIBRINOLISIS (ESTRATEGIA FÁRMACO INVASIVA)
• ICP INMEDIATA POSTERIOR A FIBRINOLISIS FALLIDA
• ICP REDUCE REINFARTO E ISQUEMIA RECURRENTE
• VENTANA DE 1.3 A 17 HORAS SEGÚN LOS ESTUDIOS:
• CAPITAL AMI, GRACIA 1, STREAM
Ibanez B, James S, Agewall S, Antunes MJ, Bucciarelli-Ducci C, Bueno H, et al. 2017 ESC Guidelines for the management of acute myocardial infarction in
patients presenting with ST-segment elevation. Eur Heart J. 2018;39(2):119–77.
36. FIBRINOLISIS-COMPARACIÓN DE FIRINOLITICO
• SE RECOMIENDAN FIBRINOESPECIFICOS
• TECNETEPLASA >ALTEPLASA
Ibanez B, James S, Agewall S, Antunes MJ, Bucciarelli-Ducci C, Bueno H, et al. 2017 ESC Guidelines for the management of acute myocardial infarction in
patients presenting with ST-segment elevation. Eur Heart J. 2018;39(2):119–77.
37. FIBRINOLISIS- TERAPIA ADYUVANTE
• DAPT:
• ASA 150-300 MG
• CLOPIDOGREL 300 MG-75 MG / >75 AÑOS 75MG-75MG
• NO HAY INFORMACIÓN DE PRASUGREL O TICAGRELOR
Ibanez B, James S, Agewall S, Antunes MJ, Bucciarelli-Ducci C, Bueno H, et al. 2017 ESC Guidelines for the management of acute myocardial infarction in
patients presenting with ST-segment elevation. Eur Heart J. 2018;39(2):119–77.
38. FIBRINOLISIS- TERAPIA ADYUVANTE
• ANTICOAGULACION
• SE PREFIERE ENOXAPARINA
• APLICAR HASTA LA REVASCULARIZACION, 8 DIAS O EGRESO
HOSPITALARIO
• ENOXAPARINA 30 MG IV -> 15 MIN DESPUÉS DOSIS SUBCUTÁNEA
1MGKG CADA 12 HRS
• >75 AÑOS SIN BOLO IV/ PRIMERA DOSIS SUBCUTÁNEA .75 MGKG MÁXIMO
75MG
• TFG<30 MISMA DOSIS PONDERAL CADA 24 HRS
• HNF: 60UIKG INFUSION 12UIKG POR 24 A 48 HRS, TPT 50-70S
Ibanez B, James S, Agewall S, Antunes MJ, Bucciarelli-Ducci C, Bueno H, et al. 2017 ESC Guidelines for the management of acute myocardial infarction in
patients presenting with ST-segment elevation. Eur Heart J. 2018;39(2):119–77.
39. FIBRINOLISIS CONTRAINDICACIONES
Ibanez B, James S, Agewall S, Antunes MJ, Bucciarelli-Ducci C, Bueno H, et al. 2017 ESC Guidelines for the management of acute myocardial infarction in
patients presenting with ST-segment elevation. Eur Heart J. 2018;39(2):119–77.
40. Manejo hospitalario
• 24 hrs de estancia en UCIC como mínimo
• 24hrs de monitoreo cardiaco
Ibanez B, James S, Agewall S, Antunes MJ, Bucciarelli-Ducci C, Bueno H, et al. 2017 ESC Guidelines for the management of acute myocardial infarction in
patients presenting with ST-segment elevation. Eur Heart J. 2018;39(2):119–77.
Notas del editor
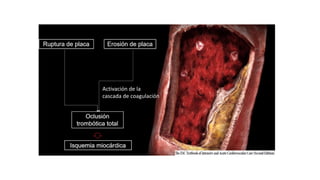
ES UN PROCESO QUE SE PERPETUA, ACTIVACION PLAQUETARIA QUE ACTIVA LA TROMBINA
600 MG DE CLOPIDOGREL ACTUAN MAS RAPIDO QUE 300 INHIBIENDO LA AGREGACION PLAQUETARIA 2 HRS TROMBOLISIS : 300 MG CADA PASTILLA VIENE DE 75 MG
Estos valores elevados de AMPc causan un estado refractario de la plaqueta y evitan los cambios conformacionales de los receptores GP IIb/IIIa, obviando la agregación plaquetaria, Así pues, el clopidogrel interfiere con las vías de señalización intraplaquetaria que conduce a la activación de la GP IIb/IIIa
El clopidogrel se convierte en el higado en su metabolito activo mediante dos etapas, que dependen de las isoenzimas del citocromo
P450 (CYP), el CYP3A4 y el CYP2C19. Ademas, la absorcion del clopidogrel (y del prasugrel) esta regulada por la glucoproteina P (codificada
por ABCB1), que es una bomba de extrusion dependiente de adenosintrifosfato (ATP) que transporta varias moleculas a traves de
las membranas extracelulares e intracelulares. Se expresa, entre otros lugares, en las celulas epiteliales del intestino, donde la expresion o la
funcion aumentadas pueden modificar la biodisponibilidad de farmacos que son sustratos.
El primer paso solo necesita esterasas plasmaticas; el segundo paso, en el higado, esta mediado por las enzimas CYP. Por consiguiente, el prasugrel produce una inhibicion plaquetaria mas rapida y constante que el clopidogre, profarmaco que bloquea de manera irreversible los receptores plaquetarios P2Y12 con una accion mas rapida y un efecto inhibidor mas profundo que el clopidogrel
No se afecta su función por los inhibidores de la bomba de protones
Este compuesto se comparo con el clopidogrel (dosis de carga de 300 mg y dosis de mantenimiento de 75 mg/dia) en el estudio TRITON-TIMI 38, en el que pacientes con SCA (IMCEST o SCASEST) programados para ICP recibieron el fármaco durante o después del procedimiento148. En los 10.074 pacientes con SCASEST incluidos en el estudio, las complicaciones CV recurrentes se redujeron en el grupo de pacientes tratados con prasugrel en el seguimiento a los 15 meses
El aumento de las complicaciones hemorragicas fue 5 veces mayor en los pacientes tratados con prasugrel referidos a CABG temprana.
Tanto prasugrel como ticagrelor tienen un inicio de acción más rápido y mayor potencia, y han demostrado ser superiores al clopidogrel en los estudios clinicos de gran tamaño
Inicio de acción mas rápido y constante que el clopidogrel, y además tiene un final de acción mas rápido, de forma que la recuperación de la función plaqueta ría es mas rápida
SI VAMOS A TORMBOLIZAR A UN PACIENTE LA SEMIVIDA DE LOS FIBRINOLITICOS ES MUY CORTA 23 A 24 MINUTOS NECESITAMOS UN COADYUVANTE EN LA ANTICOAGULACION
< 75 años 30 mg/kg IV después 1 mg/ kg SC c/12 hrs
HASTA CUANDO UTILIZAMOS LA ENOXAPARIAN, RESPUESTA : HASTA EL MOMENTO DE LA REVASCULARIZACION O EL ALTA QUE SON APROXIMADAMENTE 8 DIAS, POSTERIORMENTE LA DOSIS CAMBIA A 1 MG/KG DE PESO PERO CADA 24 HRS
Estreptocinasa = hipotensión o alergias
Alteplase = 100 mg para 90 minutos, pero lo pasamos de la siguiente manera (15 mg en bolo) y posteriormente 0.75 mg/kg de peso (max 50mg) para 30 minutos, posteriormente 0.75 mg/kg de peso que serian (35 mg) para 60 minutos ,
Tnk = mas utilizado por su administración, 0.55 mg/kg