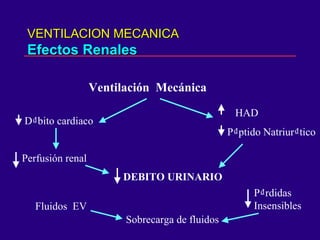
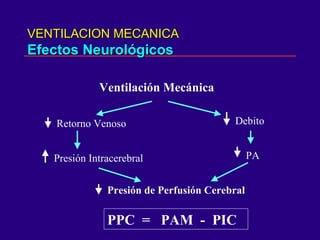
El documento describe las indicaciones y metas de la ventilación mecánica. Resume que la ventilación mecánica se usa para mejorar la ventilación alveolar y la oxigenación cuando la ventilación espontánea es inadecuada, y para disminuir el trabajo respiratorio. También describe los posibles efectos cardiovasculares, renales, gastrointestinales y neurológicos de la ventilación mecánica y cómo optimizarla para minimizar los daños.