Descargado 22 veces
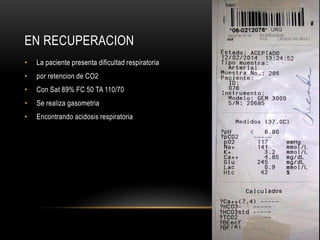

La paciente de 68 años fue ingresada para una cistolitoplaxia debido a litiasis vesical. Presenta antecedentes de cuadriplejia desde 1999 por lesión medular. La inducción anestésica fue difícil debido a la limitada apertura de la boca. Se intubó con mascarilla laríngea. El procedimiento quirúrgico fue corto. En recuperación presentó dificultad respiratoria por retención de CO2, requiriendo reintubación e ingreso a cuidados intensivos. Fue extubada después de 36 horas sin










































































