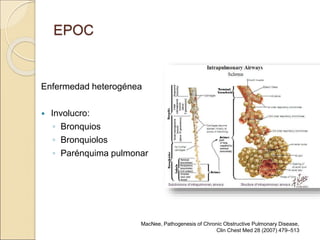
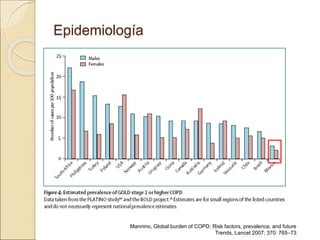
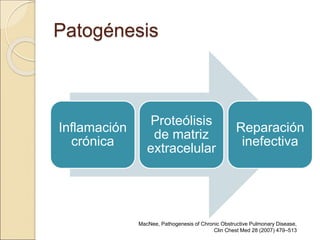
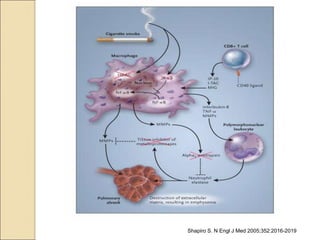
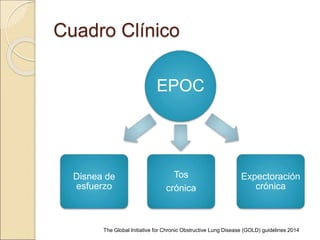
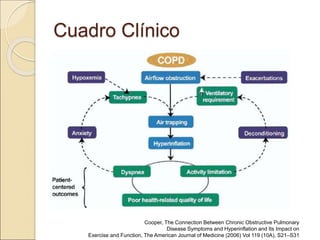
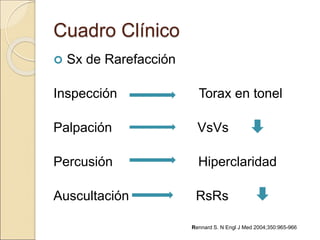
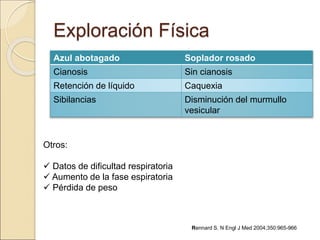
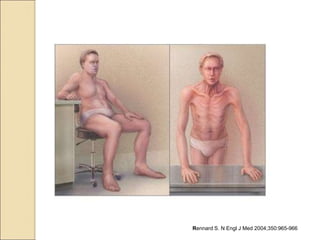
Este documento proporciona una definición y descripción general de la Enfermedad Pulmonar Obstructiva Crónica (EPOC). Explica que la EPOC se caracteriza por una limitación del flujo de aire que es progresiva y parcialmente reversible. Los principales factores de riesgo son el tabaquismo y la contaminación. El documento también cubre la epidemiología, patogénesis, cuadro clínico, diagnóstico, clasificación, tratamiento y pronóstico de la EPOC.