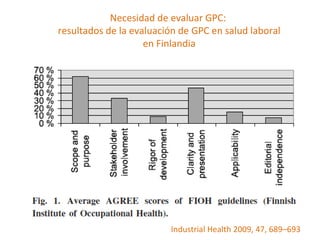
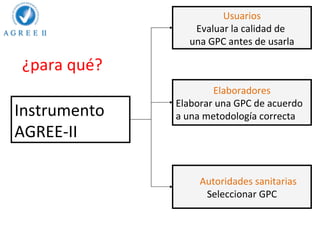
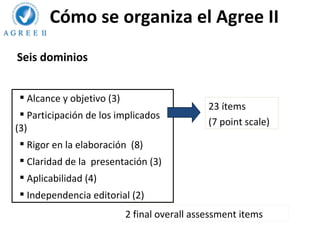
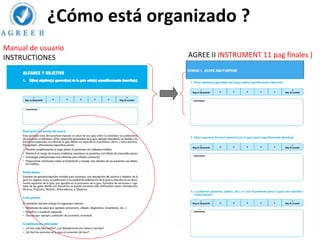
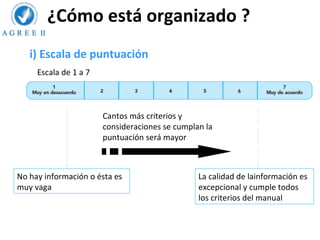
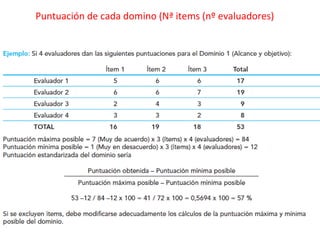
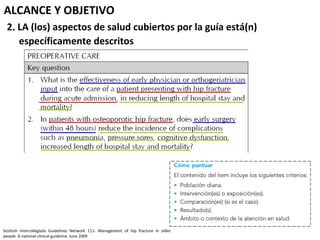
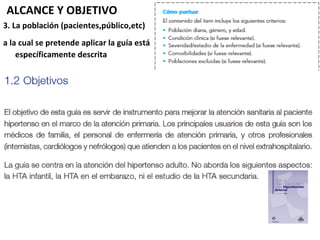
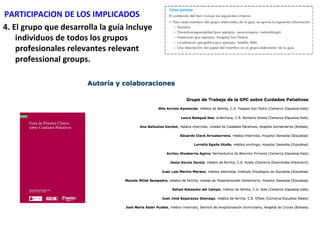
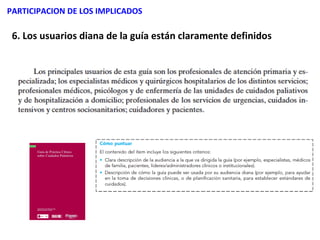
El documento proporciona una introducción al Instrumento AGREE II, el cual evalúa la calidad y rigurosidad metodológica de las guías de práctica clínica. El instrumento contiene 23 ítems agrupados en 6 dominios: alcance y objetivo, participación de los implicados, rigor de elaboración, claridad de presentación, aplicabilidad e independencia editorial. El documento explica cómo utilizar el instrumento para evaluar cada uno de los dominios de una guía clínica.