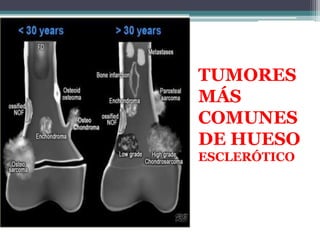
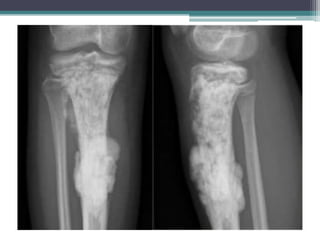
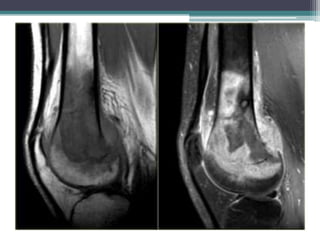
El documento resume diferentes tipos de tumores y lesiones óseas, incluyendo infarto óseo, encondroma, condrosarcoma, displasia fibrosa, metástasis, osteocondroma, osteoma osteoide, osteomielitis, osteosarcoma y fracturas por estrés. Describe las características radiológicas clave de cada una para ayudar con el diagnóstico diferencial.























































































![ATENEO TUMORES OSEOS [Autoguardado].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/ateneotumoresoseosautoguardado-251214154251-5a78dc62-thumbnail.jpg?width=640&height=640&fit=bounds)



























