Descargado 243 veces


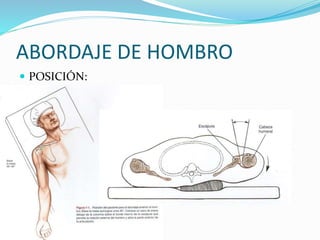














































Este documento describe los procedimientos quirúrgicos de artroscopia y abordaje del hombro. Detalla las indicaciones para abordajes anterior, posterior y artroscópicos del hombro, incluyendo la descompresión subacromial, reparación de roturas del manguito rotador y tratamiento de lesiones del labrum glenoideo. Explica los pasos quirúrgicos, como la posición del paciente, incisiones y uso del artroscopio, además de proporcionar resultados sobre el tratamiento artroscópico de artr



































































