Descargado 16 veces






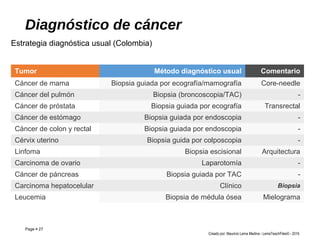
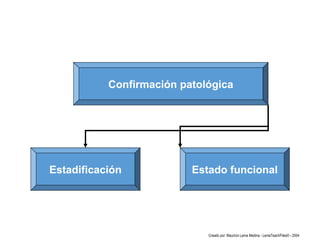
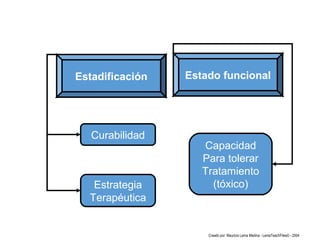










El curso de oncología para estudiantes de medicina tiene como objetivo proporcionar conocimientos sobre generalidades del cáncer, mecanismos biológicos, epidemiología y hábitos saludables para prevenirlo. Los estudiantes aprenderán a manejar emergencias oncológicas, diagnosticar y estadificar diversos tipos de cáncer, así como el enfoque terapéutico adecuado. Se aborda la importancia de la detección temprana, diagnóstico definitivo y pronóstico en los pacientes diagnosticados con cáncer.



































































