Descargar para leer sin conexión

![[ATS] Step-up randomized controlled trial of
segmental vapor ablation in patients with severe
emphysema: 6 month results
Strange CB, Herth FJF, Valipour A, Shah PL, Eberhardt R, Grah C, et al.
Mesa 4](https://image.slidesharecdn.com/mesa4-161202091058/85/Mesa-4-3-Dr-German-Peces-Barba-2-320.jpg)

![[ERS] Mepolizumab in COPD with eosinophilic
bronchitis: A randomized clinical trial
Dasgupta A, Kjarsgaard M, Capaldi D, Radford K, Aleman F, Parraga G, et al.
Mesa 4](https://image.slidesharecdn.com/mesa4-161202091058/85/Mesa-4-3-Dr-German-Peces-Barba-8-320.jpg)




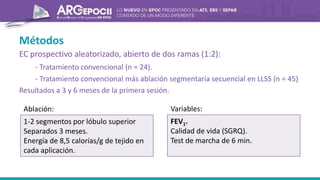
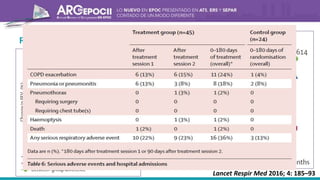
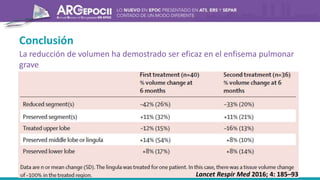
El documento describe un estudio clínico aleatorizado y controlado que evaluó la ablación por vapor segmentaria secuencial en pacientes con enfisema pulmonar grave. Los pacientes fueron asignados al tratamiento convencional o al tratamiento convencional más ablación por vapor en los lóbulos superiores en sesiones separadas por 3 meses. A los 6 meses, la ablación por vapor mejoró la función pulmonar, la calidad de vida y la capacidad de ejercicio en comparación con el tratamiento convencional solo.





























































































