El estudio encontró que:
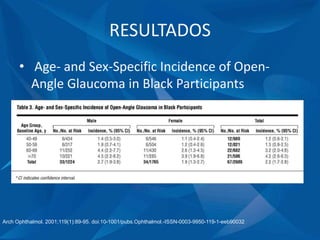
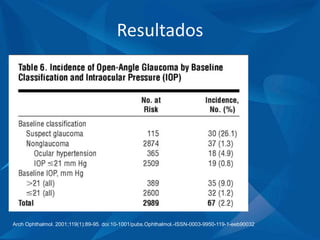
1) La incidencia de glaucoma durante un período de 4 años fue del 2.2% en personas mayores de 40 años, con 2/3 de los nuevos casos en personas mayores de 60 años.
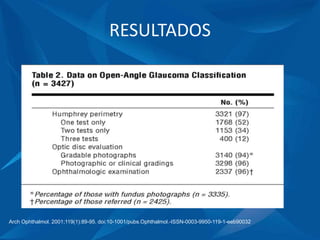
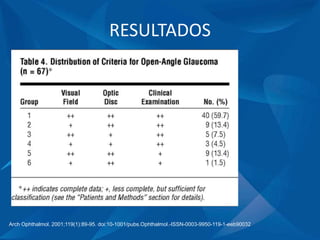
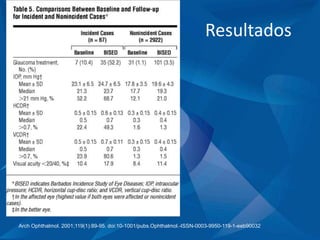
2) El 50% de los nuevos casos de glaucoma no tenían diagnóstico previo antes del seguimiento, mientras que el otro 50% ya tenía diagnóstico y tratamiento, lo que indica que el 50% de los casos de glaucoma pueden no ser detectados.
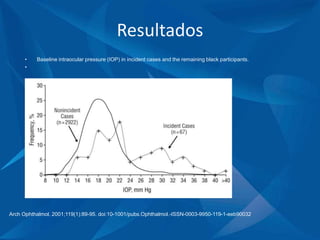
3) La presión intraocular elevada fue un factor importante en la inc








































![Causas De Disminucion De Agudeza Visual En La 2[1]Ok](https://cdn.slidesharecdn.com/ss_thumbnails/causasdedisminuciondeagudezavisualenla21ok-090712223734-phpapp02-thumbnail.jpg?width=640&height=640&fit=bounds)




























