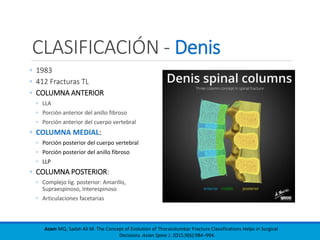
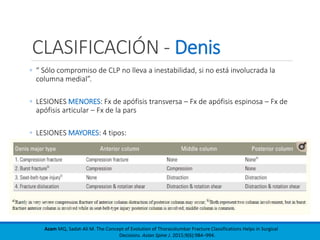
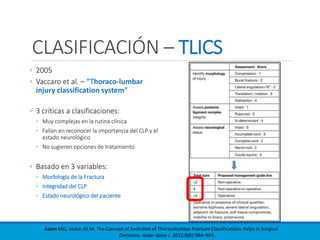
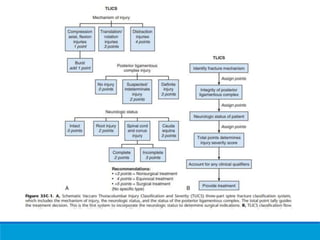
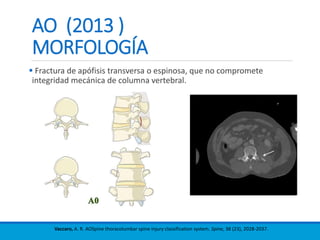
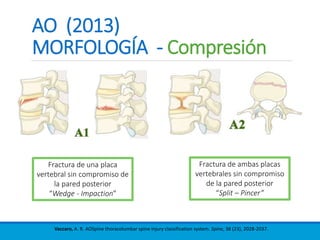
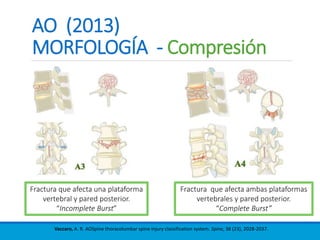
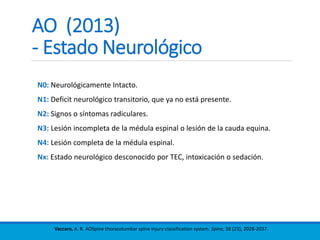
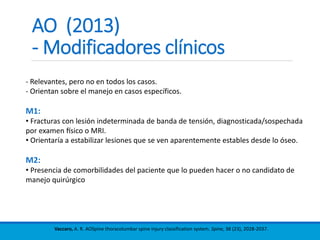
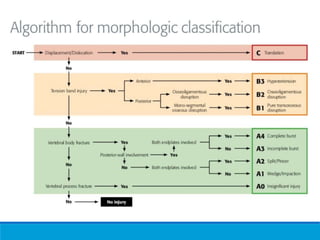
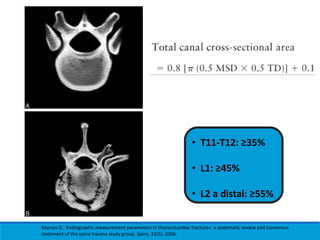
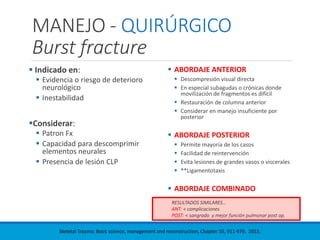
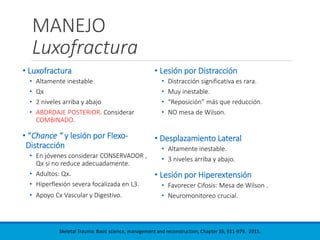
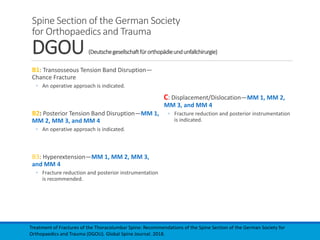
Este documento presenta una revisión de las principales clasificaciones y el manejo de las fracturas toracolumbares. Resume las clasificaciones de Boehler, Watson Jones, Holdsworth, Denis, AO/Magerl, TLICS y AO 2013, las cuales se basan en factores como el mecanismo de lesión, la integridad de las columnas vertebrales y el estado neurológico. También revisa los estudios de imagen clave para evaluar estas fracturas, como las mediciones radiográficas. Finalmente, resume las guías actuales sobre el manejo conservador y