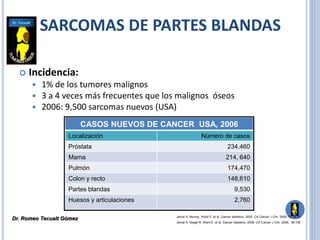
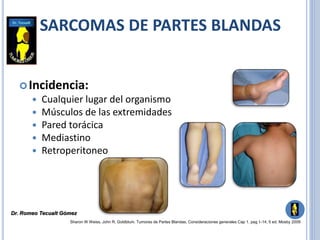
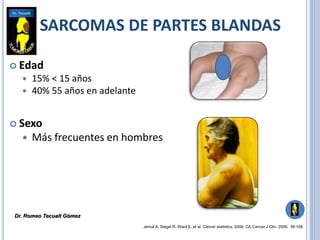
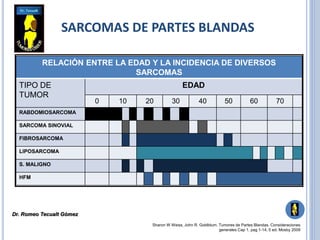
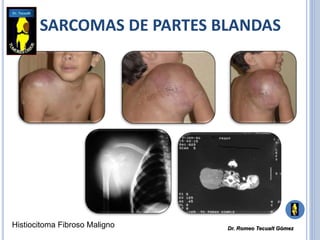
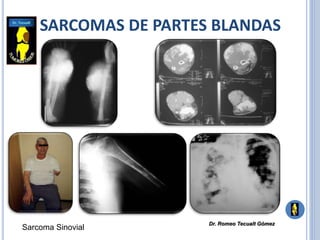
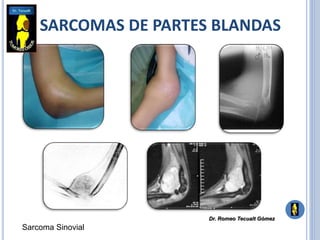
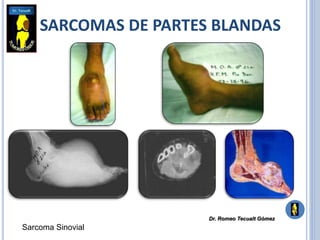
Sarcomas de partes blandas son tumores malignos que se originan en tejidos como músculo, grasa, vasos sanguíneos y tejido conectivo. Representan alrededor del 1% de todos los cánceres y son más comunes en extremidades. El tratamiento consiste principalmente en cirugía para resecar el tumor completamente con márgenes amplios, pudiendo requerir radioterapia o quimioterapia adyuvante dependiendo del tipo y grado del sarcoma.