Coroiditis serpiginosa
•Descargar como PPTX, PDF•
2 recomendaciones•2,005 vistas

La coroiditis serpiginosa afecta principalmente a personas de raza blanca y más a hombres que a mujeres. Clínicamente se presenta con lesiones de color amarillo grisáceo en forma de serpiente en la coroides interna y epitelio pigmentario de la retina. El diagnóstico se realiza mediante evaluación clínica, fotografía del fondo de ojo con fluoresceína y con indocianina verde, mostrando hipofluorescencia en las lesiones agudas y fluorescencia tardía en las lesiones crónicas.

Más contenido relacionado
La actualidad más candente
La actualidad más candente (20)
Destacado
Similar a Coroiditis serpiginosa
Similar a Coroiditis serpiginosa (20)
Más de Montemorelos
Más de Montemorelos (20)
Último
Último (20)
Coroiditis serpiginosa
- 1. 2 2 N O V I E M B R E 2 0 1 0 Coroiditis Serpiginosa Instituto de la visón Servicio de retina
- 2. Epidemiologia Mayoría son Raza Blanca Hombres > Mujeres Negros, asiáticos y Hispanos
- 3. Presentación Inicialmente un ojo afectado PIO normal BMC “casi” siempre normal Celularidad de ¼ a 1/3 en el vitreo
- 4. Presentación Clínica La lesión Coroides Interna y/o EPR Color amarillo grisáceo y apariencia difusa Forma Geográfica, bordes bien definidos Las lesiones proceden del D.O Gris Pálido en pocas semanas en forma de serpentina
- 6. Presentación Clínica CV con lesiones/Escotomas/ Rejilla Amsler Pruebas electrofisiológicas
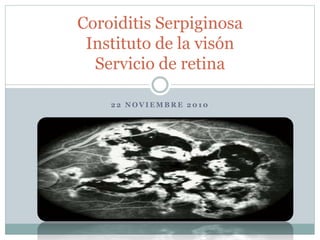
- 7. Diagnostico Evaluación Clínica FAG ICG
- 8. FAG Primera fase – Lesión aguda – Hipofluorecencia Etapas tardías – Fluoresce en zonas de lesión Lesiones agudas o crónicas hipofluorecen por la Coriocapilaris Coroides destruida Hiperfluorecencia tardía se observa en lesiones fibrosas cicatriciales
- 9. FAG
- 10. ICG Etapas Agudas – Hipofluorescencia en todas las etapas Anormalidad de los vasos coroideos o resistencia vascular coriocapilar
- 12. Diagnostico Diferencial Multifocal posterior placoid pigment epitheliopathy (AMPPPE) CNV Histoplasmosis ocular Degen. Macular Toxoplasmosis Escleritis Posterior Coroiditis multifocal Sarcoidosis Linfoma no Hodgking’s Tumor metatasico Osteoma Coroideo
- 14. Tratamiento
- 17. FAG ICG
- 18. PREGUNTAS Y COMENTARIOS
Notas del editor
- coroiditis serpiginosa, también llamada coroidopatía geográfica helicoidal peripapilar o coroiditis geográfica, es una enfermedad rara, generalmente bilateral, enfermedad inflamatoria crónica recurrente de causa desconocida coroides y la retina (EPR) Px. De Mediana Edad y Adultos pero tb se presenta en jovenes
- Negros, asiáticos y Hispanos sin manifestaciones sistémicas o asociación con las drogas, trauma o allergy No hay propensión familiar conocido
- A veces el paciente solo percibe una disminucion de la AV cuando involucra Macula y cuando se afecta el ojo contralateral Compromiso Foveal disminuye la AV reacción inflamatoria de camara anterior no granulomatosa
- Estas lesiones pueden crecer no sólo hacia el disco (fig. 105-2D), sino también peripherally.8 personas con coroiditis serpiginosa macular puede tener un peor pronóstico visual y diagnóstico preciso y el tratamiento rápido son primordiales. La neovascularización coroidea (NVC) puede ocurrir en asociación con coroiditis serpiginosa Un ojo puede tener una lesión macular aguda, mientras que el otro puede tener un peripapilar lesion.5 Del mismo modo, un ojo puede tener la CNV, mientras que el otro sólo puede tener cambios inflamatorios agudos
- FAG A, Red-free fundus photograph of the left macula of a 54-year-old white man. Note sensory detachment of the macula (arrows), subretinal hemorrhage centrally, and a geographic scar in the papillomacular bundle. B, Arteriovenous-phase fluorescein angiogram of the left macula. Note the patch of subretinal neovascularization in the central macula (arrows). The geographic lesion is in the papillomacular bundle. C, Late arteriovenous-phase fluorescein angiogram of the left macula. Note staining of the geographic lesion in the papillomacular bundle and fuzzy fluorescence of the subretinal neovascularization in the macula, which is leaking fluorescein under the sensory retinal detachment of the macula. D, Red-free fundus photograph of the right macula. The small, active inflammatory geographic lesion just temporal to the macula has "glowing" acute inflammatory edges (arrows).
- Los resultados de las pruebas electrofisiológicas son generalmente normales, aunque en casos muy graves en los que grandes áreas del fondo de ojo se ven afectadas, un electrorretinograma anormal o anormal oculogram electro-puede ser recorded.2
- Atrophic lesions show diffuse loss of pigment, choroidal vessels, and late staining on fluorescein angiography. Laboratory evaluation of these patients is invariably unrewarding. An association of serpiginous choroiditis and tuberculosis has been suggested. However, treatment with antimicrobial agents has made no difference to the course of the disease in these patients.[27]
- La fluorescencia por lo general comienza desde el borde de la lesión y se extiende hacia el interior. La angiografía es bastante típica, mostrando la imagen total de "dedos" del tejido afectado. Esto contrasta con la fluorescencia de la CNV, que muestra de encaje, irregular y nodular hiperfluorescencia en las fotos de fase temprana
- A, Red-free fundus photograph of the left macula of a 50-year-old white man. Note the acute geographic inflammatory lesion in the macula and papillomacular bundle (arrows). B, Early arteriovenous-phase fluorescein angiogram of the left macula. Note hypofluorescence of the acute inflammatory lesion. C, Late-phase fluorescein angiogram of the left macula. Note staining of the acute inflammatory lesion. D, Red-free fundus photograph of the left macula 4 months later. Note the scarring of the older geographic lesion in the macula and the fresh inflammatory lesion (arrow) extending superonasal from the macula in the upper part of the papillomacular bundle. E, Arteriovenous-phase fluorescein angiogram of the left macula. Note new acute lesions in the upper part of the papillomacular bundle. F, Late-phase fluorescein angiogram of the left macula. Note mild staining of the old inflammatory lesion in the macula and more intense fluorescent staining of the new inflammatory lesion in the upper part of the papillomacular bundle.
- También puede haber áreas localizadas de hiperfluorescencia fuera de estas zonas. Estas últimas lesiones no se corresponden con los cambios clínicamente visible de la retina, EPR, o de la coroides y podría representar áreas de la forma subclínica coroidea inflammation. Giovani y al. Sugirieron un sistema de clasificacion combinado de FAG y ICG
- FAG A, Red-free fundus photograph of the left macula of a 51-year-old white man. An extensive acute geographic inflammatory lesion extends from the optic nerve head and involves much of the central, lower, and temporal macula, as well as the upper part of the papillomacular bundle. The only area seemingly not involved is the upper macula. B, Early arteriovenous-phase fluorescein angiogram of the left macula. Note hypofluorescence of the acute inflammatory lesion in the macula and papillomacular bundle. C, Late-phase fluorescein angiogram of the left macula. Note staining of the geographic lesion in the macula. D, Note leakage of the retinal vein below the macula (phlebitis, arrow) overlying the acute inflammatory lesion. E, Red-free fundus photograph of the left macula 1 year later. The acute inflammatory geographic lesion in the upper part of the macula has extended to involve the entire macular area. Vision has been markedly reduced. F, Fluorescein angiogram of the left macula. There is extensive involvement of the entire macular and papillomacular bundle area.
- A number of inflammatory diseases can mimic serpiginous choroiditis.21 The condition that most resembles serpiginous choroiditis is acute multifocal posterior placoid pigment epitheliopathy (AMPPPE). Although AMPPPE can affect only one eye, with the fellow eye unaffected until a later date, in most instances both eyes are affected at the same time. In addition, AMPPPE does not usually recur; if it does, it is usually within the first few weeks or months of its initial presentation. Recurrences of AMPPPE do not happen over the course of years, as in serpiginous choroiditis. Finally, permanent vision loss in AMPPPE is unusual.
- A, Red-free fundus photograph of the left posterior pole of a 40-year-old white man. Large geographic areas of atrophy extend in a propeller-like fashion from the optic nerve head. The lesion just skips the left fovea (arrow). Note also the pigment epithelial hyperplasia. B, Early arteriovenous-phase fluorescein angiogram of the left posterior pole. Lesions show large choroidal vessels but no choriocapillaris; these are old lesions with absent choriocapillaris and pigment epithelium. C, Later arteriovenous-phase fluorescein angiogram of the left posterior pole. There is staining along the edges of the lesions. D, Late arteriovenous-phase fluorescein angiogram of the left nasal mid-periphery. Lesions extend out from the disc. Unattached lesions (arrows) show skipped areas.
- There are no reports of successful management of CNV associated with serpiginous choroiditis with anti-inflammatory agents. Thermal laser has been the main form of therapy for extrafoveal or juxtafoveal CNV.1,13,14 Recurrence after laser has been reported.11 Subfoveal CNV due to serpiginous choroiditis may be amenable to verteporfin photodynamic therapy but there are no reports describing results to date. Body_ID: P105028 Patients with serpiginous choroiditis are instructed to perform frequent Amsler grid testing to monitor for the presence of recurrent disease or CNV. Because similar central vision changes can occur with either, patients are instructed to return for immediate examination and angiography when symptoms occur.
- A, Red-free fundus photograph of the left macula of a 51-year-old white man. The atrophic geographic lesion extends from the optic nerve head and involves the central, temporal, and lower parts of the macula. B, Arteriovenous-phase fluorescein angiogram. The choriocapillaris and pigment epithelium are gone, as evidenced by the visibility of large choroidal vessels within the lesion. C, Late-phase fluorescein angiogram of the left macula. Note staining along the edges of the geographic lesion.
- The fellow eye of the patient shown in Figure 105-4. A, Red-free fundus photograph of the right posterior pole. Large lesions extend from the optic nerve head and involve the macula (arrow). This eye had a marked reduction in visual acuity. Note the scarring and pigment epithelial hyperplasia. B, Arteriovenous-phase fluorescein angiogram of the right posterior pole. Large choroidal vessels within lesions show that the choriocapillaries and pigment epithelium are gone. There is hyperfluorescence along the edges of the lesions. C, Late arteriovenous-phase fluorescein angiogram of the posterior pole, right fundus. There is early staining along the edges of the lesion and staining of the fibrous scar (arrow). D, Late arteriovenous-phase fluorescein angiogram of the right eye, superonasal area. Note the finger-like projections extending toward the mid-periphery.
- A, Clinical photograph demonstrating a creamy yellow lesion in the central macula, representing the macular variant of serpiginous choroidopathy. B, Early-phase fluorescein study demonstrating hypofluorescence of the acute lesion. The margins of the lesion are not well demarcated. C, Late-phase fluorescein study demonstrating intense hyperfluorescence and staining of the lesion. D, Early-phase indocyanine green (ICG) study demonstrating marked hypofluorescence of the lesion. Overlying retinal vessels are visualized, but all detail of the underlying choroidal vasculature is lost. E, Late-phase ICG study demonstrating persistent hypofluorescence and well-demarcated margins of the lesion. F, Very-late-phase ICG study demonstrating persistent hypofluorescence of the lesion and a halo of hyperfluorescence along its margin. Also note the focal, intense hyperfluorescent spots that may represent sites of subclinical choroidal inflammation.
- VISUAL PROGNOSIS Significant loss of central and even peripheral vision can occur as a result of inflammatory disease and its sequelae. Frequencies of central vision loss have been reported to be as high as 50% of involved eyes.7,8,32 This is especially true in patients with macular serpiginous choroiditis. In addition, CNV can occur in up to 25% of patients. Nevertheless, most patients with serpiginous choroiditis maintain central function in at least one eye.