Descargado 194 veces








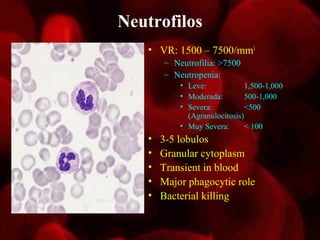



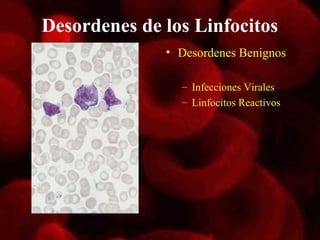


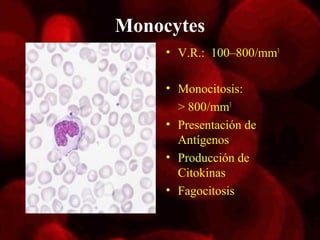




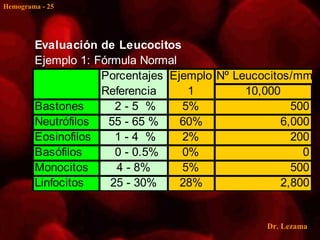




Este documento resume los componentes principales de un hemograma, incluyendo eritrocitos, leucocitos, plaquetas y sus valores de referencia normales. Describe las etapas de la eritropoyesis y las funciones de los eritrocitos. Explica los índices eritrocitarios y los rangos normales para hemoglobina, hematocrito y recuento de eritrocitos. Luego resume los tipos de leucocitos, sus porcentajes normales y desórdenes asociados con leucocitosis y leucopenia. Finalmente, cubre los rangos normal








![Cirrosis ..[1]](https://cdn.slidesharecdn.com/ss_thumbnails/cirrosis-1-120404134159-phpapp02-thumbnail.jpg?width=640&height=640&fit=bounds)
































![Catalogo hema [autoguardado]](https://cdn.slidesharecdn.com/ss_thumbnails/catalogohemaautoguardado-141110211654-conversion-gate02-thumbnail.jpg?width=640&height=640&fit=bounds)













































