Manejo Médico de Síntomas Urinarios Bajos y Crecimiento Prostático
•Descargar como PPT, PDF•
0 recomendaciones•657 vistas

Más información en: urowoller.com

Recomendados
Recomendados
Más contenido relacionado
La actualidad más candente
La actualidad más candente (20)
Destacado
Destacado (17)
Similar a Manejo Médico de Síntomas Urinarios Bajos y Crecimiento Prostático
Similar a Manejo Médico de Síntomas Urinarios Bajos y Crecimiento Prostático (20)
Más de Uro Woller
Más de Uro Woller (20)
Último
Último (20)
Manejo Médico de Síntomas Urinarios Bajos y Crecimiento Prostático
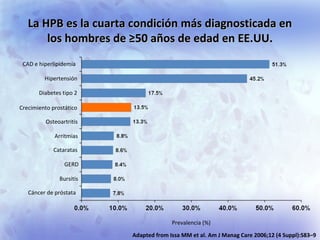
- 1. La HPB es la cuarta condición más diagnosticada enLa HPB es la cuarta condición más diagnosticada en los hombres de ≥50 años de edad en EE.UU.los hombres de ≥50 años de edad en EE.UU. Prevalencia (%) CAD e hiperlipidemia Hipertensión Diabetes tipo 2 Crecimiento prostático Osteoartritis Arritmias Cataratas GERD Bursitis Cáncer de próstata Adapted from Issa MM et al. Am J Manag Care 2006;12 (4 Suppl):S83–9
- 2. Los hombres de mayor edadLos hombres de mayor edad son afectados comúnmente por SVUBson afectados comúnmente por SVUB moderados a graves atribuibles a la HPBmoderados a graves atribuibles a la HPB 1. Roehrborn CG et al. BJU Int. 2007;100:813–9. 2. EAU Guidelines on BPH www.uroweb.org La prevalencia de la HPB histológica es de 50% en los hombres de 51-60 años de edad y aumenta a 90% en aquellos de 81-90 años de edad1 La prevalencia de los síntomas moderados a graves varía de 14 a 30%2
- 3. Naturaleza progresiva de HPB no tratadaNaturaleza progresiva de HPB no tratada 1. Djavan et al. Curr Opin Urol 2004; 44: 45. 2. McConnell et al. N Engl J Med 2003; 349: 2387. Consecuencias de progresión de HPB: ■ Deterioro de síntomas ■Impacto negativo en la calidad de vida ■Desarrollo de complicaciones ■Necesidad de interveción quirúrgica Marcadores clínicos de alto de riesgo de progresión incluyen :1 • Aumento volumen prostático (>30 cm3 ) • PSA >1.4 ng/ml • Edad >50 años • Severidad de LUTS MTOPS: Incidencia acumulada de progresión clínica de17% para grupo placebo vs. 5% para hombres tratados con combinación de finasteride y doxazosina2
- 4. La mayoría de los pacientes buscaLa mayoría de los pacientes busca asesoramiento médico debido a laasesoramiento médico debido a la molestia que les causan sus síntomasmolestia que les causan sus síntomas Hutchison A et al. Eur Urol. 2006;50:555–61.
- 5. Factores de riesgo/ condiciones comórbidas Mecanismo Edad Disfunción Vascular Diabetes, Síndrome metabólico Obesidad, Sedentarismo Hiperactividad adrogénica, Estimulación Insulínica Disfunción Vascular Enfermedad cardiovascular Hipertensión Disfunción Vascular Reducción en señales ON Condiciones Inflamatorias Secreción de citoquinas de las células epitelio/estromales Andersson KE et al. Neurourol Urodyn (2011); 30(3):292-301.Andersson KE et al. Neurourol Urodyn (2011); 30(3):292-301. Factores de Riesgo LUTS/ HPB/ DEFactores de Riesgo LUTS/ HPB/ DE
- 6. Progresión clínica en HPBProgresión clínica en HPB McConnell et al. New Engl J Med 2003; 349: 2387. Progrescióndelaincidenciaacumulativa(%) 5.01.0 1.5 2.0 2.5 3.0 3.5 4.0 4.5 5.50.0 0.5 25 20 15 10 5 0 Años de la selección al azar Incidencia acumulada de progresión clinica a 4 años* = 17% Evolución de la enfermedad en el brazo placebo de MTOPS** destaca la naturaleza progresiva de HPB *Progresión clínica definida como un incremento ≥4 points desde el basal en el score de síntomas AUA (IPSS), retención aguda de orina, incontinencia urinaria , insuficiencia renal o infección urinaria recurrente
- 7. El deterioro de los síntomasEl deterioro de los síntomas es la manifestación más comúnes la manifestación más común de progresión de la HPBde progresión de la HPB Incidencia acumulativa de eventos de progresión en el brazo de placebo a los cuatro años en el estudio de Tratamiento Médico de los Síntomas Prostáticos (MTOPS) Aumento de ≥ 4 puntos en la calificación de síntomas de la AUA Retención urinaria aguda (RUA) Incontinencia Infección de vías urinarias (IVU) o urosepsis McConnell JD et al. N Engl J Med. 2003;349:2387−98.
- 8. El PSA basal más alto estuvo asociado con unEl PSA basal más alto estuvo asociado con un aumento de los eventos de progresión de la HPBaumento de los eventos de progresión de la HPB en el estudio MTOPSen el estudio MTOPS Crawford ED et al. J Urol. 2006;175:1422–7. 3.1 2.8 0.3 0.8 5.9 4.5 1.0 1.8 0.0 2.0 4.0 6.0 8.0 p=0.0002 p=0.0281 p=0.029 p=0.018 Tasadeincidencia (eventosporcada100años-paciente) Progresión global de la HPB Progresión de ≥ 4 puntos en el índice de síntomas de la AUA RUA Tratamiento invasivo <1.6 ng/ml ≥1.6 ng/ml Concentración de PSA
- 9. Estudios que establecen la HPB como unaEstudios que establecen la HPB como una condición progresivacondición progresiva Olmstead County Study (USA) 471–2115 42 meses–6 años Baltimore Long Study of Aging 537 Cross-sectional MTOPS 3047 5.5 años Forth Valley Study (Scotland) 217 3 años Veterans Affairs Hospitals (USA) 556 60 meses Health Professionals Study (USA) 6100 Cross-sectional Urology Practice Study (USA) 500 4 años 2-Year Combined Finasteride Data 4222 2 años The PLESS Study (USA) 3040 4 años Estudio n Seguimiento Múltiples estudios epidemiológicos y brazos pacebo de estudios clínicos (ej. MTOPS) confirman que la HPB es una condición progresiva
- 10. La BPH es una condición muy comúnLa BPH es una condición muy común ◦ European Commission eurostat database. Available at: http://epp.eurostat.ec.europa.eu/portal/page/portal/population/data/database. Accessed 24 January 2012 at 11:30 GMT; 2. Hutchison et al. Eur Urol 2006;50:555–562. 2010 Hasta 24 millones de hombres en la EU1,2 >50 años de edad se encuentran afectados por STUI moderados a severos debidos a HPB
- 11. Fuente: CIA World Factbook Julio 19, 2012
- 12. SOURCE: U.S. Census Bureau, Current Population Survey, Annual Social and Economic Supplement, June 2011.
- 13. Total 112,336,538.00 54,855,231.0054,855,231.00 HombresHombres 50 a 54 años 5,064,291.00 2,402,451.00 55 a 59 años 3,895,365.00 1,869,537.00 60 a 64 años 3,116,466.00 1,476,667.00 65 a 69 años 2,317,265.00 1,095,273.00 70 a 74 años 1,873,934.00 873,893.00 75 a 79 años 1,245,483.00 579,689.00 80 a 84 años 798,936.00 355,277.00 85 y más años 703,295.00 298,739.00 Total de hombres mayores de 50 años 8`951,5268`951,526 16,32% del total de hombres son mayores de 50 años16,32% del total de hombres son mayores de 50 años 7,96% del total de la población7,96% del total de la población Fuente INEGI - Censo al 12 de Junio de 2010 Población masculina en México INEGI 2010
- 14. Fuente: Consejo Nacional de Población, Proyecciones de la población de México 2010 – 2050. Noviembre 2012
- 15. Impacto económico de HPBImpacto económico de HPB Fenter et al. Am J Man Care 2006; 12: S90. Consecuencias de HPB como RAO y cirugía repesentan un problema de salud pública de alto impacto econónico. (USD). CAD: coronary artery disease; GERD: gastroesophageal reflux disease
- 16. Unidades por clase Terapéutica 2011 Tratamiento médico de la HPB:Tratamiento médico de la HPB: Venta de fármacos a nivel mundialVenta de fármacos a nivel mundial IMS Health, Diciembre 2011 Mercado Privado de Farmacias
- 17. Unidades por Clase Terapéutica 2011 IMS Health, Diciembre 2011 Mercado Privado de Farmacias Tratamiento médico de la HPB:Tratamiento médico de la HPB: Uso de fármacos a nivel mundialUso de fármacos a nivel mundial
- 18. 72% 66% 69% 89% 86% 93% 68% 70% 68% 82% 72% 71% 22% 25% 14% 7% 9% 7% 19% 14% 19% 14% 28% 21% 0% 0% 0% 4% 4% 0% 4% 0% 3% 0% 0% 1% 6% 9% 17% 0% 1% 0% 8% 16% 10% 4% 0% 7% 0% 20% 40% 60% 80% 100% Arg Bra C.Ame Chi Col Ecu Mex Per R.Dom Uru Ven LA α-Bloq 5ARI α-Bloq+5ARI Other Tratamiento médico de la HPB:Tratamiento médico de la HPB: Uso de fármacos a nivel deUso de fármacos a nivel de Latino América y por paísLatino América y por país IMS Health, Diciembre 2011 Mercado Privado de Farmacias Unidades por clase Terapéutica 2011
- 19. Andersson KE et al. Neurourol Urodyn (2011); 30(3):292-301. ● Proliferación de células epiteliales y estromales. ● Factor de crecimiento celular. ● Ambiente androgénico alterado. ● Predisposición genética. ● Reducción de niveles NO. ● Incremento de actividad Rho-quinasa. ● Hiperactividad autonómica. ● Inflamación. ● Disminución en perfusión sanguínea secundaria a aterosclerosis e isquemia. Fisiopatología de Hiperplasia Prostática Benigna/ Sintomatología Urinaria
- 20. 1. Rosen CR et al. Eur Urol (2005); 47:824–37. 2. Somlyo AP et al. J Physiol (2000); 522(2):177–85. 2. Taylor JM et al. Asian J Androl (2008); 10(1):45–53. La Rho/Rho-quinasa se encuentra involucrada en la regulación adrenérgica en la contracción de músculo liso en vas deferens, próstata y pene. El incremento de la Rho/Rho-quinasa relacionada con la edad de ha demostrado en modelo animal. •El incremento de la actividad de la Rho/Rho-quinasa resulta en incremento en la contracción de músculo liso de próstata y pene con el posterior proceso obstructivo de vaciamiento vesical y DE respectivamente. •Los inhibidores de Rho/Rho-quinasa en modelos animales disminuyen las contracciones adrenérgicas y la proliferación de músculo liso prostático. El incremento de la Rho/Rho-quinasa es un posible mecanismo común en la patogénesis de HPB-LUTS y DE. Incremento de activación Rho-quinasaIncremento de activación Rho-quinasa
- 21. Andersson KE et al. Neurourol Urodyn (2011); 30(3):292-301. Reducción de niveles NOS/OSReducción de niveles NOS/OS ● La relajación del músculo liso del tracto urinario inferior es debido al óxido nítrico endotelial. ● Disminución de la relación NOS/NO promueve la proliferación de células de músculo liso en próstata y vejiga con la posterior presentación de Síntomas Urinarios Bajos. ● Estudios animales muestran que la inhibición de producción de NO promueve la hiperactividad vesical e incrementa el tono de la glándula prostática. ● Estos factores tienen efecto de la disfunción endotelial en la patogénesis de los Síntomas Urinarios.
- 22. 1. Mc.Vary K. BJU Intl (2006); 97(2):23–8. 2. Taylor JM et al. Asian J Androl (2008); 10(1):45–53. 3. Andersson KE et al. Neurourol Urodyn (2011); 30(3):292-301. Aterosclerosis PélvicaAterosclerosis Pélvica ● Posible hipótesis relacionada a patogénesis de LUTS y Disfunción eréctil. ● Hipoperfusión sanguínea crónica de la vejiga, próstata y pene; mayor riesgo de LUTS. • Disminución en transmisión de señales de eNOS relacionadas con la edad causada por disfunción vascular. • Hiperactividad vesical.
- 23. 23/51 Inervación autonómica del tono de músculo lisoInervación autonómica del tono de músculo liso 1.1. Rosen CR et al. Euro Urol (2005); 47:824–37.Rosen CR et al. Euro Urol (2005); 47:824–37. 2.2. Taylor JM et al. Asian J Androl (2008); 10(1):45–53.Taylor JM et al. Asian J Androl (2008); 10(1):45–53. Subtipos de receptores α-Adrenérgicos y localización Receptor Localización [12–17]. α-1A Células estromales prostáticas, músculo liso vascular, uretra, vas deferens, vejiga. α-1B Células estromales prostáticas, músculo liso vascular. α-1D Células estromales prostáticas, uretra, vas deferens, vejiga, músculo detrusor. α-1 y α-2 Vasculatura peneana, músculo liso de cuerpo cavernoso.
- 24. ● HPB proceso histológico caracterizado por hiperplasia de las células estromales y epiteliales, inicialmente en zona periuretral de la próstata. ● Los andrógenos factor importante en el crecimiento de la próstata. ● DHT es el andrógeno más abundante dentro de la glándula. ● Incremento de la concentración local de DHT se relaciona con incremento prostático. Androgenos (DHT) Androgenos (DHT) Agonista Agonista Proliferación Celular Muerte Celular Muerte Celular Antagonista Antagonistia Balance Desbalance TGFβ TGFβKGF EGF IGFs KGF EGF IGFs Próstata Normal Hiperplasia Prostática HPB= Hiperplasia prostática benigna; DHT = dihidrotestosterona; EGF = factor crecimiento epidérmico; ERb = receptor b de endotelina ; IGF =tipo insulina; KGF = factor crecimiento keratinocito; LUTS = Sintomatología urinaria baja; TGF =factor crecimiento trandformador 1. Rosen CR et al. Eur Urol (2005); 47:824–837. 2. Alonso-Magdalena P et al. PNAS (2009); 106(8):2859-2863 Proliferación Celular Control molecular del crecimiento prostático
- 25. PROBE:PROBE: los pacientes seleccionarían un fármaco quelos pacientes seleccionarían un fármaco que redujera los efectos a largo plazoredujera los efectos a largo plazo Adapted from Emberton M. Int J Clin Pract 2010;64:1425–1435. 75% de los pacientes preferiría un fármaco que pudiera reducir el riesgo de cirugía en un 50% versus un fármaco que proporcionara un alivio de los síntomas más rápido 75% de los pacientes preferiría un fármaco que pudiera reducir el riesgo de cirugía en un 50% versus un fármaco que proporcionara un alivio de los síntomas más rápido Pacientes de 45–80 años de edad que recibieron medicamentos de prescripción para la HPB (n=502), urológos (n=100) Cuestionario basado en la encuesta que cubre las creencias y las percepciones sobre la HPB y su tratamiento. 40 30 20 10 0 1 2 3 4 5 6 7 8 Calificación 35% 17% 17% 8% 6% 6% 5% 5% Porcentajedepacientes Reducción del 50% en el riesgo de Cirugía; alivio de síntomas en 6 meses Alivio de los síntomas en 2 semanas, sin ninguna reducción en el riesgo de cirugía
- 26. Encuesta de HPB: una perspectiva masculinaEncuesta de HPB: una perspectiva masculina ◦ La encuesta en línea de 1,161 hombres europeos con síntomas urinarios molestos1 ◦ Los hombres tuvieron una edad de ≥ 50 años de Alemania, Francia, Italia, España y UK1 ◦ La Encuesta de la HPB: una perspectiva masculina explora: • Los síntomas experimentados • Lo que desmotiva a los hombres de buscar asesoría médica • Lo que motiva a los hombres a buscar ayuda • Con quiénes hablan los hombres sobre sus síntomas urinarios molestos BPH survey, Accessed from http://www.ismh.org/en/press-corner/ 28 January 2012.
- 27. Encuesta de HPB: los hombres se mostraron renuentes a buscarEncuesta de HPB: los hombres se mostraron renuentes a buscar asesoría sobre sus síntomas urinariosasesoría sobre sus síntomas urinarios BPH survey: Accessed from http://www.ismh.org/en/press-corner/ 28 January 2012. 46% de los hombres nunca había discutido sus síntomas con un doctor
- 28. ◦ Los hombres esperarían casi 2 años para buscar asesoría médica en relación a sus síntomas urinarios De aquellos que no buscaron asesoría médica: ◦ 64% creyó que sus síntomas eran una parte inevitable de envejecer ◦ 40% aceptaría sus síntomas urinarios en vez de ver a un doctor ◦ Sólo 14% pensó que su doctor podría mejorar sus síntomas ◦ Para la mayoría de los hombres con un diagnóstico de HPB, muchos lo recibieron conforme mencionaban sus síntomas “de pasada” BPH survey: Accessed from http://www.ismh.org/en/press-corner/ 28 January 2012. Encuesta de HPB: los hombres se mostraron renuentes a buscarEncuesta de HPB: los hombres se mostraron renuentes a buscar asesoría sobre sus síntomas urinariosasesoría sobre sus síntomas urinarios
- 29. Encuesta de HPB: conclusionesEncuesta de HPB: conclusiones ◦ Los hombres no relacionan los síntomas urinarios con problemas de la próstata • Los problemas de la próstata y los síntomas necesitan mencionarse de forma proactiva con el paciente ◦ Existe una necesidad de comunicación abierta entre los pacientes y los médicos • Los problemas de la próstata deben abordarse como cualquier otra condición crónica ◦ Disipar los mitos sobre los problemas urinarios • Los síntomas urinarios molestos no son una parte inevitable del envejecimiento • El tratamiento es efectivo para controlar los síntomas BPH survey: Accessed from http://www.ismh.org/en/press-corner/ 28 January 2012.
- 30. Por lo general a los pacientes les preocupan losPor lo general a los pacientes les preocupan los riesgos a largo plazo y no los síntomas de lariesgos a largo plazo y no los síntomas de la HPBHPB ◦ Cuestionario nacional de US basado en hombres (n=419) con HPB moderada a severa : ◦ 70% estaban más preocupados por los riesgos a largo plazo que por los síntomas ◦ 64% estaban dispuestos a esperar hasta 3 meses para obtener un beneficio en los síntomas si se alcanzaba un tratamiento a largo plazo ◦ 76% estaban dispuestos a tomar dos medicamentos para reducir el tamaño de la próstata y obtener una mejoría en los síntomas Kaplan S et al. Int J Clin Pract 2006;60:1157–1165.
- 31. La mayoría de los hombres estaban más preocupados por los riesgos a largoLa mayoría de los hombres estaban más preocupados por los riesgos a largo plazo de la HPB que por los síntomas inmediatosplazo de la HPB que por los síntomas inmediatos Kaplan S et al. Int J Clin Pract 2006;60:1157–1165. Adapted from Emberton M. Int J Clin Pract 2010;64:1425–1435 80 70 60 50 40 30 20 10 0 Pacientes con síntomas ligeros (n=216) Urólogos (n=100)Médicos de atención primaria (n=100) Pacientes con síntomas moderados o severos (n=203) De alguna manera de acuerdo Fuertemente de acuerdo 10% 35% 35% 37% 35% 21% 5% 32% Proporción de pacientes y doctores que estuvo de acuerdo en que los pacientes están más preocupados por el efecto a largo plazo La mayoría de los médicos creyó que los pacientes estaban más preocupados por el alivio inmediato de los síntomas que por los efectos a largo plazo
- 32. Comprensión de los médicos de los tratamientos paraComprensión de los médicos de los tratamientos para la HPBla HPB Porcentaje que está de acuerdo con la declaración Urólogos MPC Los 5ARI son efectivos para reducir el tamaño de la próstata 52% 19% Los 5ARI son efectivos para detener la progresión de la enfermedad 40% 21% Los α-bloqueadores son efectivos para reducir el tamaño de la próstata 1% 5% Los α-bloqueadores son efectivos para detener la progresión de la enfermedad 4% 10% Encuesta telefónica de US a 100 urólogos y 100 MPC. Kaplan S et al. Int J Clin Pract 2006;60:1157–1165. Respuestas a las preguntas en la encuesta de Kaplan. Es menos probable que los MPC conozcan los beneficios a largo plazo de los 5ARIEs menos probable que los MPC conozcan los beneficios a largo plazo de los 5ARI MPC-Médicos de Primer Contacto.
- 33. Preferencias de los médicos hacia los tratamientosPreferencias de los médicos hacia los tratamientos para la HPBpara la HPB ◦ Los resultados del estudio PROBE encontraron que 63% de los urólogos prescribieron una terapia con fármacos a más de 70% de sus pacientes ◦ Los factores que se consideraron importantes para elegir la terapia del fármaco incluyeron: • Volumen prostático (68% de los urólogos) • Evidencia de progresión de la enfermedad (66% de los urólogos) ◦ 78% de los urólogos pensaron que los 5ARI reducirían el riesgo de progresión de la HPB ◦ 44% de los urólogos pensaron que los α-bloqueadores reducirían el riesgo de progresión Emberton M. Int J Clin Pract 2010;64:1425–1435.
- 34. Expectativas para el tratamiento de la HPB: resumenExpectativas para el tratamiento de la HPB: resumen ◦ Las preferencias de los médicos y los pacientes para el tratamiento de la HPB no se encuentran alineadas • Las preferencias de los pacientes son hacia los beneficios a largo plazo1,2 • Los patrones de prescripción de los médicos son hacia los beneficios en los síntomas2 ◦ Los Urólogos y los Médicos de Primer Contacto tienen una comprensión diferente en relación a la eficacia de las terapias con fármacos para prevenir la progresión de la HPB1,2 1. Kaplan S et al. Int J Clin Pract 2006;60:1157–1165; 2. Emberton M. Int J Clin Pract 2010;64:1425–1435.
- 35. ConclusionesConclusiones ◦ La HPB es una condición1 muy común y una enfermedad progresiva2 ◦ La identificación de los factores de riesgo proporciona la base de un enfoque orientado hacia el perfil de riesgos para el control de la HPB • El APE y el volumen prostático son indicadores poderosos de la progresión de la HPB3 • 3 de 4 pacientes diagnosticados con HPB tuvieron un crecimiento prostático (>30 cc)4,5,6 ◦ Las preferencias de los médicos y los pacientes para el tratamiento de la HPB no se encuentran alineadas • Las preferencias de los pacientes son hacia beneficios a largo plazo7,8 y los patrones de prescripción de los médicos son hacia beneficios en los síntomas8 ◦ La severidad de los STUI puede afectar de forma adversa áreas importantes de las relaciones personales 9 1. European Commission eurostat database. Available at: http://epp.eurostat.ec.europa.eu/portal/page/portal/population/data/database. Accessed 24 January 2012 at 11:30 GMT; 2. Hutchison et al. Eur Urol 2006;50:555–562; 2.. Adapted from McConnell J et al. New Engl J Med 2003;349:2387–2398; 3 Roehrborn CG. Int J Impot Res 2008;20 (Suppl 3):S19–26; 4. Carballido J et al. Int J Clin Pract 2011;65:989–996; 5. GSK data on file D-IMPACT CSR; 6. Nickel J et al. Can Urol Assoc J 2008;2:367–373. 7. Kaplan S et al. Int J Clin Pract 2006;60:1157–1165; 8. Emberton M. Int J Clin Pract 2010;64:1425– 1435; 9. Roehrborn CG et al. Prostate Cancer Prostatic Dis 2006;9:30–34
- 36. Evolución de las recomendaciones para el tratamientoEvolución de las recomendaciones para el tratamiento de la HPBde la HPB ◦ 1. AUA guidelines on the management of BPH (1994) http://www.auanet.org/; 2. de la Rosette JJ et al. Eur Urol 2001;40:256–263; 3. AUA. J Urol 2003;170:530–547; 4. Madersbacher S et al. Eur Urol 2004;46:547–554; 5. NICE clinical guideline 97 (2010). Available at: http://guidance.nice.org.uk/ 6. AUA. Management of BPH (2010) http://www.auanet.org/; 7. Oelke M et al. Guidelines on the treatment of non- neurogenic male LUTS, incl. Benign Prostatic Obstruction (BPO) (2012). http://www.uroweb.org/; 8. Lepor H et al. N Engl J Med 1996;335:533– 539; 9. Debruyne F et al. Eur Urol 1998;34:169–175; 10. McConnell J et al. N Engl J Med 2003;349:2387–2398; 11. Kirby R et al. Urology VA Co-op8 (finasterida + terazosina) ALFIN9 (finasterida + alfuzosina) PREDICT11 (finasterida + doxazosina) MTOPS10 (finasterida + doxazosina) Datos de 2 años del CombAT12 (dutasterida + tamsulosina) Datos de 4 años del CombAT13 (dutasterida + tamsulosina) Guías5,6 de la AUA y el NICE de 2010 Guías7 de la EAU de 2012 Guías3 de la AUA de 2003 Guías4 de la EAU de 2004 Guías1 de la AUA de 1994 Guías2 de la EAU de 2001 20052000 2012 El tratamiento de primera línea recomendado para hombres con HPB en riesgo de progresión es una terapia combinada de un 5ARI más un α-bloqueador El tratamiento de primera línea recomendado para hombres con HPB en riesgo de progresión es una terapia combinada de un 5ARI más un α-bloqueador
- 37. EAU BPH guidelines Oelke M, et al. Eur Urol 2012 Evaluación en Hombres con LUTSEvaluación en Hombres con LUTS
- 38. Roehrborn C.19th Congreso Asociación Europea de Urología. Viena, Austria.2004 ALGORITMO PARA EL MANEJO MÉDICO DE LA HBPALGORITMO PARA EL MANEJO MÉDICO DE LA HBP
- 39. * FITOTERAPIA: No recomendada, sin embargo su uso es basado en experiencia del médico tratante. (") ESTUDIOS ESPECIALES: Se realizarán a juicio de un urólogo previa valoración del tratamiento médico. (-) De acuerdo a disponibilidad y comorbilidades del paciente y de la experiencia del médico tratante. Rev Mex Urol 2012;72(Suplemento 1):22-42 FLUJOGRAMA DE GUÍAS CLÍNICAS PARA EL MANEJO DEL CRECIMIENTO PROSTÁTICO Dr. Mauricio Cantellón Orozco
- 40. Tratamientos farmacológicos actuales (EAU)Tratamientos farmacológicos actuales (EAU) Recomendado? ◦ Observación activa (Watchful waiting) ◦ Bloqueadores-Alfa ◦ Antimuscarínicos ✓ ◦ Inhibidores de 5-alpha-reductasa (5ARIs) ◦ Fitoterapia x ◦ Vasopresina (nicturia por poliuria nocturna) ✓ ◦ Terapia combinada ✓ ◦ Inhibidores PDE5 (LUTS+ disfunción eréctil) ✓ EAU BPH guidelines Oelke M, et al. Eur Urol 2012
- 41. La fitoterapia es poco aconsejableLa fitoterapia es poco aconsejable • Las diferencias en componentes y técnicas de obtención de los extractos de plantas impiden la comparación de los diversos preparados • Los estudios aleatorizados a corto plazo sugieren que algunos preparados son eficaces y seguros • No existen resultados de estudios bien diseñados, de largo plazo y controlados con placebo • Se necesitan estudios adicionales que sigan las recomendaciones de la Consulta Internacional Chatelain C, et al. Proceedings 5th International Consultation on BPH (2001) *EAU BPH guidelines Oelke M, et al. Eur Urol 2012 El comité de directrices no es capaz de hacer recomendaciones específicas acerca de la fitoterapia debido a la heterogeneidad de los productos y los problemas metodológicos asociados con los meta - análisis
- 42. Tratamiento del crecimiento prostático y susTratamiento del crecimiento prostático y sus síntomas. Guías Mexicanas.síntomas. Guías Mexicanas. ◦ 1) Vigilancia Activa. Educacional . Ne-1B. ◦ 2) Fitoterapia. Comité Mexicano –sin recomendación de uso para HBP. Gr rec–A. ◦ 3) Alfa-bloqueadores. Primera línea Ne-1A ◦ 4) 5ARIs. Primera línea. Ne-1B. Gr rec A. ◦ 5) Combo 5Ari-alfabloq. Ne-1B. Gr rec A.
- 43. Tratamiento HBP. Guías MexicanasTratamiento HBP. Guías Mexicanas ◦ 6)6) IPDE5. Beneficio Clínico. Coexistencia STUI-DE. Ne-1B. Gr. rec A ◦ 7)7) Antimuscarínicos. Síntomas de almacenamiento. Ne-1B. Gr rec B Precaución en obstrucción de salida Ne-4. Gr rec C.
- 44. Tratamiento Quirúrgico. Guías MexicanasTratamiento Quirúrgico. Guías Mexicanas ◦ RTUP sigue siendo el “estándar de oro”. ◦ Cirugía abierta ◦ Laparoscópica. ◦ Robótica. ◦ ITUP (tuip) ◦ Laser ◦ Ablación ◦ HIFU
- 45. Objetivos de la terapia farmacológica en HPBObjetivos de la terapia farmacológica en HPB Reducir complicaciones serias Impacto en la enfermedad suyacente reduciendo el volúmen prostático Mantener y/o mejorar el flujo de orina a largo plazo Mejoría de síntomas LUTS y reducir las molestias en el largo plazo Prevenir la progresión de HPB
- 46. Razonamiento de la terapia combinadaRazonamiento de la terapia combinada 5AR2 5AR1 Finasteride Dutasteride Reducción VP 5AR2 Relajación músculo liso 5ARIs α-bloquedores La terapia combinada ofrece rápido y duradero alivio de síntomas y reducción a largo plazo de la progresión
- 47. Finasterida Dutasterida Inhibición de la 5αR tipo I x0 x45 Inhibición de la 5αR tipo II x1 X2.5 Supresión sérica de DHT 70% 93% Vida media 6-8 h 5 Semanas Reducción del volumen prostático (%) -18 -26 Reducción de síntomas (IPSS) 3.3 4.5 Mejoría del flujo Qmax (mL/s) 1.9 2.2 Reducción de retención urinaria 1.8 3 Cirugía por HPB 2.2 5 Efecto adverso, disfunción eréctil 3-4 1-6 Efecto adverso, disminución de libido 4-5 4 Efecto adverso, anormalidad de eyaculación 4-5 1-2 Rev Mex Urol 2012;72(Suplemento 1):22-42 Tabla que compara las características de ambos inhibidores de la 5α- reductasa disponibles en la actualidad
- 48. 5-ARI y5-ARI y αα-bloqueadores recomendados como-bloqueadores recomendados como tratamientos de primera líneatratamientos de primera línea 1. Oelke M et al. Guidelines on the treatment of non-neurogenic male LUTS, incl. Benign Prostatic Obstruction (BPO) (2012). http://www.uroweb.org/; 2. NICE clinical guideline 97 (2010) http://guidance.nice.org.uk/; 3. Castineiras Fernandez J et al. Actas Urol Esp 2010;34:24–34; 4. Molero García JM, et al. Criterios de derivación en hiperplasia prostática benigna para Atención Primaria, versión 2011. Aten Primaria. 2011. doi:10.1016/j.aprim.2011.07.006; 5. AUA. Management of BPH (2010) http://aunet.org/; 6. Nickel J et al. Can Urol Assoc J 2010;4:310–316. EAU (2012)1 NICE (UK, 2010)2 AEU (España, 2010/11)3,4 AUA (2010)5 CUA (Canadá, 2010)6 LUTS m-s, crecimiento prostático (>40 cm3 ) y Qmax bajo (apropiados únicamente para tratamiento a largo plazo; es decir ≥1 año) LUTS m-s molestos y próstata >30 g o PSA >1.4 ng/ml IPSS moderada (8– 20), PV alto en DRE o >30 cm3 y PSA >1.5 ng/ml LUTS con crecimiento prostático (medición del volumen, PSA como una variable para el volumen y/o DRE) LUTS con crecimiento prostático La AUA y la CUA recomiendan una combinación para próstatas “agrandadas” mientras que la EAU, el NICE y la AEU proporcionan recomendaciones precisas.
- 49. Terapia combinadas en LUTS/HPBTerapia combinadas en LUTS/HPB Mayores estudios clinicos disponiblesMayores estudios clinicos disponibles • VA COOP4 (1996) • Finasteride 5 mg /dia más terazosin 5–10 mg/dia por 1 año (n=1229) • ALFIN1 (1998) • Finasteride 5 mg/dia más alfuzosina 5 mg c/12 hrs por 6 meses (n=1051) • MTOPS2 (2003) • Finasteride 5 mg/dia más doxazosina 4–8 mg/dia por un por undemedio de 4.5 años (n=3047) • PREDICT3 (2003) • Finasteride 5 mg/día más doxazosin 4–8 mg / dia por 1 año (n=1095) • CombAT5 (2010) • Dutasteride 0.5 mg/dia más tamsulosin 0.4 mg /dia por 4 años (n=4844) 1. Debruyne et al. Eur Urol 1998; 34: 169; 2. McConnell et al. N Engl J Med 2003; 349: 2387. 3. Kirby et al. Urology 2003; 61: 119; 4. Lepor et al. N Engl J Med 1996; 335: 533. 5. Roehrborn et al. Eur Urol 2010; 57: 123.
- 50. Nuevos tratamientosNuevos tratamientos ◦ Terapia Génica ◦ I COX-2 / LOX-2 ◦ Análogos Vitamina D Elocalcitol BXL-628 ◦ IPDE5-UK369003 ◦ Neurotoxina Botulínica Tipo A. ◦ NX-1207 • Fase III. Inicialmente para Alzheimer con dosis única tiene efectos significativos. Proapoptósico Ind J Pharmacol 2011;43:6-12 50/51
- 52. "Los hombres deberían discutir sus opciones con sus médicos antes de someterse a tamizaje. Los hombres que gozan de buena salud y tienen una esperanza de vida de 10-15 años deberían tener la opción de someterse a exámenes y no ser desanimados de hacerlo. La declaración general de la USPSTF (United States Preventive Services Task Force) no debería ser aplicada a las poblaciones de rio, como los riesgo como los afroamericanos”. AUA.
- 53. Arthur SchopenhauerArthur Schopenhauer La salud no es todo,La salud no es todo, pero sin ella, lo demáspero sin ella, lo demás es nadaes nada
Notas del editor
- Un estudio retrospectivo naturalista evaluó las 10 enfermedades diagnosticadas más prevalecientes en hombres mayores de 50 años de edad empleando los datos sobre reclamos de la base de datos Integrated Health Care Information Solutions (IHCIS) National Managed Care Benchmark (que incluye datos de 30 planes de salud de US que cubren más de 25 millones de vidas).1 Las enfermedades más comunes diagnosticadas en hombres ≥50 años de edad a partir de los datos de la IHCIS fueron enfermedad arterial coronaria (CAD)/hiperlipidemia, seguidas de hipertensión, diabetes tipo 2, crecimiento prostático y osteoartritis, respectivamente.1 Referencia 1. Issa MM et al. Am J Manag Care 2006;12 (4 Suppl):S83–9.
- Los datos recolectados por el proyecto de Investigación Transeuropea del Uso de las Políticas de Manejo de los SVUB sugerentes de HPB en la Atención Primaria de la Salud (TransEuropean Research Into the Use of Management Policies for LUTS suggestive of BPH in Primary Health care [TRIUMPH]) fueron utilizados para establecer el perfil de 4,979 pacientes de seis países europeos que se presentaron recientemente con SVUB / HPB a médicos generales o urólogos basados en consultorios. 1 La mayoría de los pacientes (77%) buscaban asesoramiento médico debido a las molestias que les causaban sus síntomas.1 Referencia 1. Hutchison A et al. Eur Urol 2006;50:555–61.
- Row 4 of Table (“Inflammatory Conditions”) -- secretion of cytokines such as interleukin-8 by epithelial or stromal cells.
- Estos datos muestran la frecuencia de los eventos de progresión en el estudio MTOPS (Tratamiento Médico de los Síntomas Prostáticos), lo cual demuestra que el más común de todos fue un aumento de por lo menos 4 puntos en la calificación de los síntomas de acuerdo con la AUA.1 Referencia 1. McConnell JD et al. N Engl J Med 2003;349:2387−98.
- El estudio de Tratamiento Médico de los Síntomas Prostáticos (MTOPS) fue un estudio en gran escala, doble ciego, en el que 3,047 hombres con HPB fueron aleatorizados a recibir 5.0 mg de finasterida, 4.0 u 8.0 mg de doxazosina, una combinación de finasterida y doxazosina, o placebo, y fueron seguidos durante un periodo promedio de 4.5 años.1 Se hizo un análisis de los datos del brazo de placebo del estudio MTOPS para identificar los predictores clínicos de la progresión de la HPB.2 El volumen prostático estuvo entre los factores basales que se encontró eran predictivos de progresión de la HPB.2 El riesgo de progresión de la HPB (un criterio de valoración combinado definido como un aumento arriba de la evaluación basal de por lo menos 4 puntos en la Calificación de Síntomas de la Asociación Urológica Norteamericana, RUA, incontinencia urinaria, insuficiencia renal o infección recurrente de vías urinarias) fue significativamente mayor en los pacientes tratados con placebo con un APE basal de 1.6 ng/mL o mayor contra un APE de menos de 1.6 ng/mL.2 Referencias McConnell JD et al. N Engl J Med 2003;349:2387–98. Crawford ED et al. Urology 2006;175:1422–7.
- At least nine studies involving &gt;20,000 men have provided evidence for the progressive nature of BPH. The minimum follow-up in the seven non-cross-sectional studies was 2 years.
- This slide presents a list of conditions and factors that may contribute to the pathology of benign prostatic hyperplasia (BPH) and lower urinary tract symptoms (LUTS).
- Bulletpoint 1 (Rho/Rho-kinase pathway) This pathway starts with Rho, a small monomeric G-protein that activates Rho-kinase. Activated Rho-kinase inhibits the myosin phosphatase, an enzyme that dephosphorylates the myosin regulatory light chain (RLC), and thus inhibits myosin II and contraction. As a result of the inhibition of the myosin phosphatase, these downstream events are prevented, and the resulting increase in RLC phosphorylation leads to contraction. Bulletpoint 3 – These observations support the role of increased Rho/Rho-kinase activity as a possible common mechanism for the pathogenesis of LUTS and ED in BPH.
- Endothelial nitric oxide (NO) inhibits the tone of smooth muscles in LUT resulting in their relaxation. When compared with normal prostate tissue, nitrergic innervation is significantly reduced in prostatic tissue of patients with benign prostatic hyperplasia (BPH).
- Pelvic atherosclerosis may also play a key role in the pathogenesis of both LUTS and ED in patients with BPH. Bulletpoint 3 – one factor that leads to altered blood supply in the LUT may be due to decreased endothelial nitric oxide synthase (eNOS) signaling with advancing age. Bulletpoint 4 – activation of hypoxia inducible factor (HIF) reduces cellular apoptosis and increases the levels of growth factors such as vascular endothelial growth factor (VEGF), transforming growth factor-b and cytokines such as interleukin-8, causing increased stromal proliferation and LUTS. Bulletpoint 5 – in animal models of BOO, ischemia was found to be associated with reactive oxygen species, causing bladder overactivity. This may be due to activation of capsaicin sensitive C-fiber afferent pathways.
- Kaplan et al indican que cuando se pregunta específicamente a los pacientes sobre el riesgo a largo plazo versus el alivio de los síntomas, declaran que es más probable que se preocupen por el riesgo a largo plazo (y esto contrasta con la visión de los clínicos) [Kaplan et al Int J Clin Pract 2006;60:1157–65].
- Various treatment options are available for men with LUTS suggestive of BPO. Of all the potential treatment approaches available, only phytotherapy is not recommended in current EAU BPH guidelines.
- The ultimate goal of medical therapy in patients with BPH is the prevention of disease progression. Additional therapeutic goals may include: impacting on the underlying disease process by reducingprostate volume improving and maintaining urinary flow over the long term improving LUTS and reducing bothersome symptoms over thelong term reducing serious BPO/BPE-related complications.
- Given their complementary modes of action, combination therapy with a 5ARI and an α-blocker should lead to rapid improvements in symptoms and significant reductions in the risk of long-term adverse outcomes, such as acute urinary retention (AUR) and BPH-related surgery. Dutasteride in combination with an α-blocker targets the α1-adrenoceptors, 5AR1 and 5AR2. Combination therapy with the type 2-selective 5ARI, finasteride, and an α-blocker targets only the 5AR2 receptors and α1-adrenoceptors.