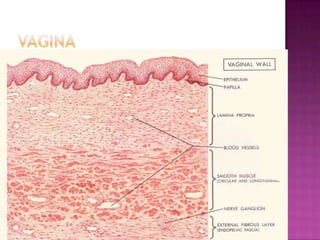
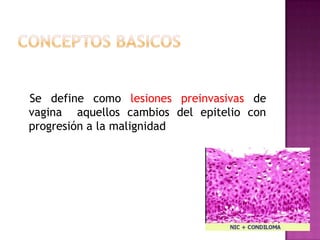
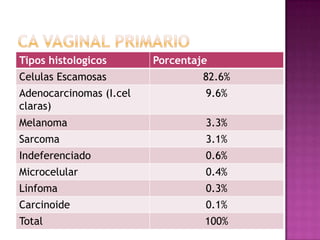
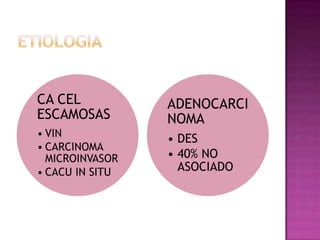
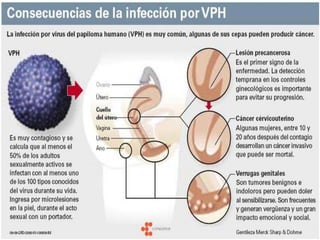
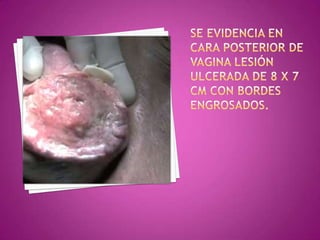
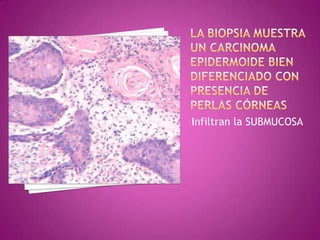
Este documento describe lesiones preinvasivas y canceres de vagina. Define hiperplasia, metaplasia y displasia como lesiones preinvasivas que pueden progresar a cáncer. Explica que la mayoría de cánceres de vagina son metastáticos de cáncer de cuello uterino o vulva, y que los virus del papiloma humano (VPH) causan alrededor del 90% de cánceres de vagina. Resume los síntomas, tipos histológicos, estadios y tratamientos de cáncer de vagina





































































![Cuello Del Utero[1]](https://cdn.slidesharecdn.com/ss_thumbnails/cuellodelutero1-091106093632-phpapp01-thumbnail.jpg?width=640&height=640&fit=bounds)









































