Descargado 266 veces
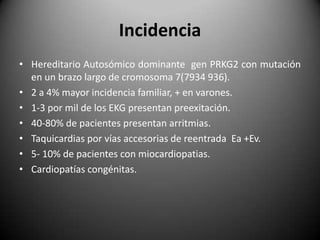
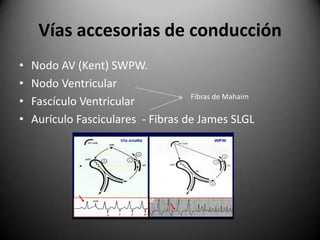
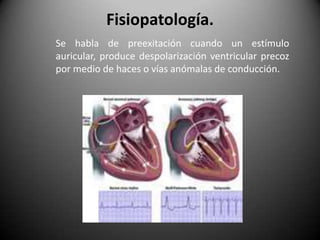

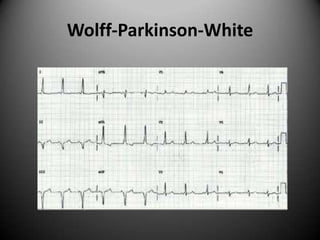

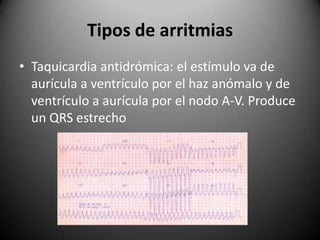


Este documento resume la enfermedad de Wolff-Parkinson-White, una afección cardíaca hereditaria caracterizada por la presencia de vías accesorias de conducción que causan una conducción anómala entre las aurículas y los ventrículos. Se detallan la incidencia, las vías accesorias más comunes, los síntomas, los hallazgos en el electrocardiograma, los tipos de arritmias asociadas y los enfoques de diagnóstico y tratamiento, incluida la ablación por catéter de radiofrecuencia























































































