Descargado 119 veces














![(83 x edad (años) - (43 x Indice Barthel)
MODELOS DE PREDICCIÓN CLÍNICA
Age Ageing (2014) 43 (3): 346-351
Rev Med Chile 2014; 142: 826-832
Escala de validación de delirium incidental.
2 estudios prospectivos observacionales (desarrollo 375 ptes y validación 104
ptes).Pacientes hospitalizados de más de 65 años
AUC 0.86 (IC 95% 0.82- 0.91) LR (-) 0.16 LR (+) 3.4
Validación AUC 0.78 ( 95% IC 0.66 -0.90)
Valor -240 VPN: 0.99 E: 74% S: 88%
Score >- 240 Aumenta la probabilidad post test a 45%
Delirium predictive score (DPS)
= [1370 × BUN (mmol/l)/cr (umol/l)] – (4 × Barthel index) Corte -240
= [5 × BUN (mg/dl)/cr (mg/dl)] – (3 × Barthel index) Corte -160
Escala de validación para predecir pacientes con alto riesgo de delirium
2 estudios prospectivos observacionales (desarrollo 542 ptes y validación 85 ptes)
Pacientes hospitalizados de más de 65 años
Después de las 48 h de hospitalización.
Análisis multivariado : edad y estado funcional
AUC 0.83 (IC 0.73 -0.92)
Bajo riesgo: < 1700
Riesgo intermedio 1700-3000
Alto >riesgo 3000](https://image.slidesharecdn.com/delirium-190612033254/85/Delirium-19-320.jpg)
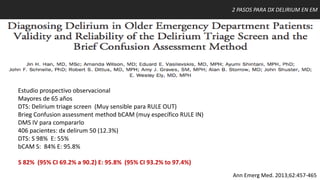
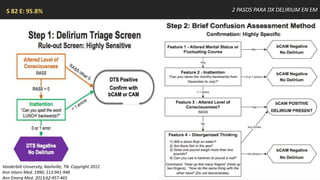

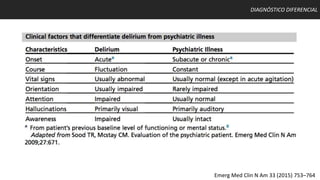


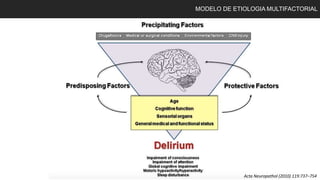
1. El delirium es un síndrome de inicio agudo con alteraciones en la atención, conciencia y cognición, con un curso fluctuante. 2. Los factores de riesgo incluyen edad avanzada, comorbilidades, deterioro cognitivo previo y estados críticos. 3. La evaluación incluye escalas como CAM, CAM-ICU y ICDSC, con CAM teniendo alta sensibilidad y especificidad.























































































