Descargado 733 veces






















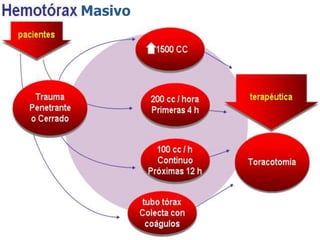



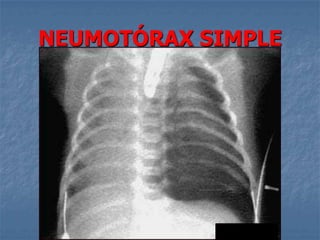







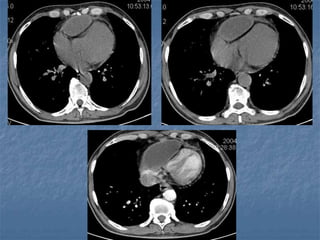















1. El documento describe diferentes tipos de lesiones por trauma de tórax, incluyendo aquellas que ponen en peligro la vida de forma inmediata como obstrucción de la vía aérea, neumotórax a tensión y hemotórax masivo, y aquellas que pueden matar de forma mediata como neumotórax simple y contusión pulmonar. 2. Se explican los síntomas, diagnóstico y tratamiento de cada lesión, haciendo énfasis en la evaluación y estabilización inicial del paciente mediante la re


































































































