Descargado 405 veces














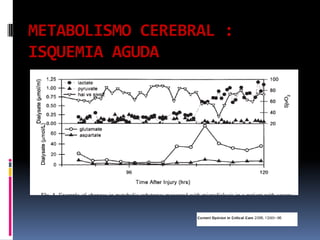











Este documento resume conceptos fisiológicos del sistema nervioso central. Explica que el cerebro recibe el 15-20% del gasto cardiaco a pesar de solo representar el 2-3% del peso corporal. Describe las teorías de la autorregulación cerebral y factores que la afectan como la presión de perfusión cerebral. Finalmente, analiza alteraciones del flujo sanguíneo cerebral en traumatismos craneoencefálicos e isquemia y su relación con el metabolismo cerebral.










![1 hipertension endocraneana[1]](https://cdn.slidesharecdn.com/ss_thumbnails/1hipertensionendocraneana1-121026194735-phpapp02-thumbnail.jpg?width=640&height=640&fit=bounds)










































































