Descargado 193 veces
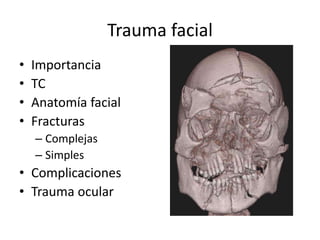
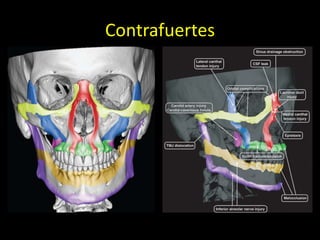
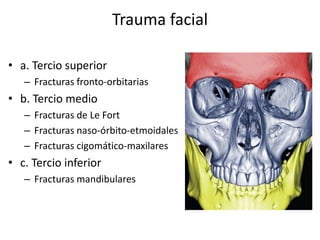
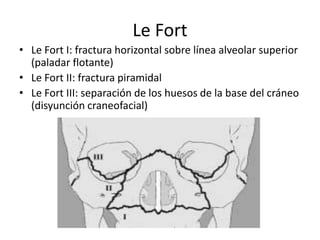
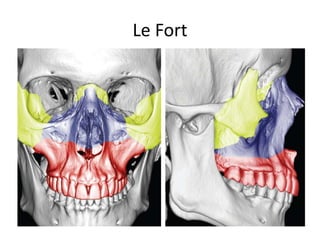
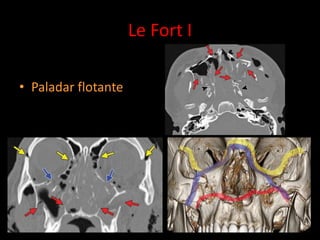
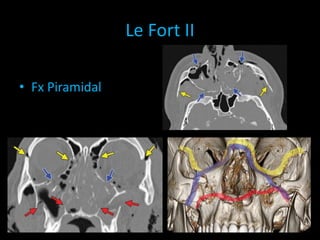
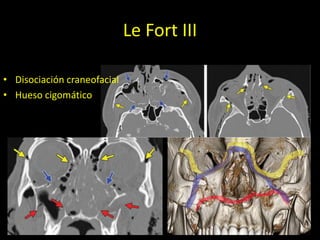
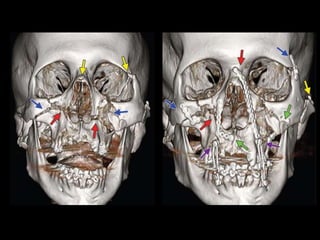
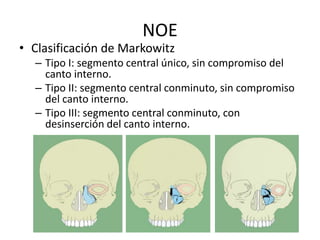
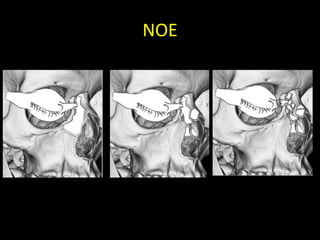

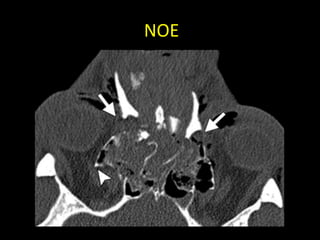
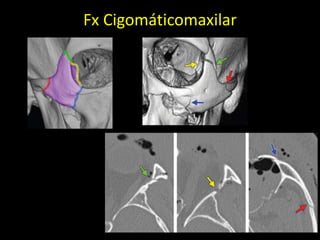
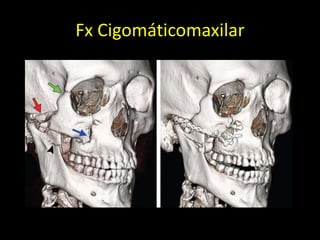
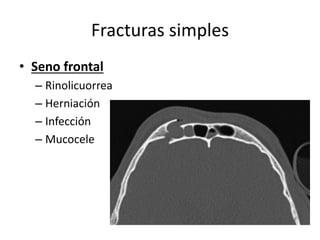
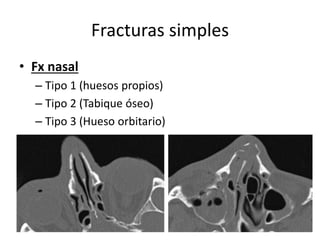
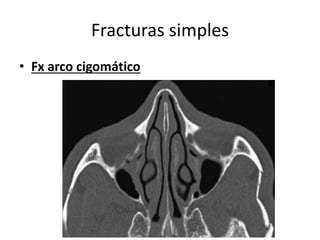
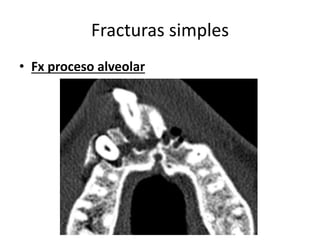
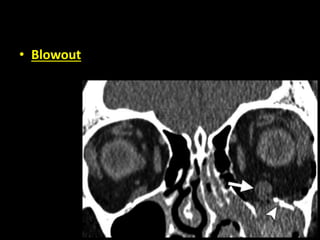
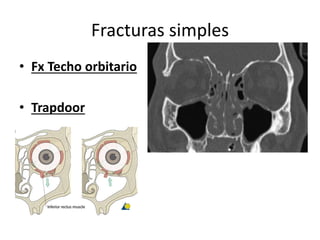
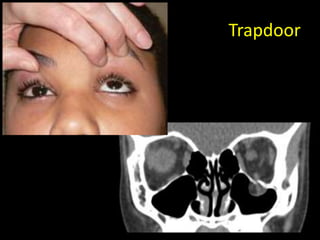
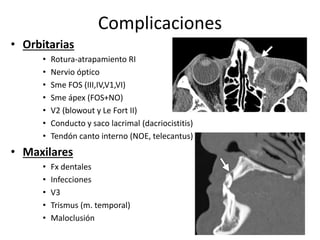
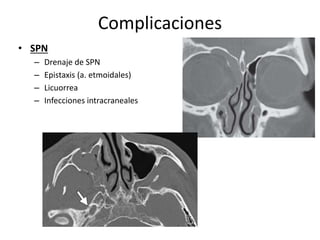
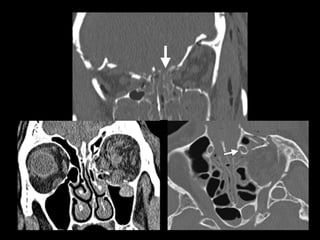
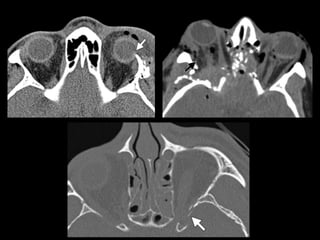
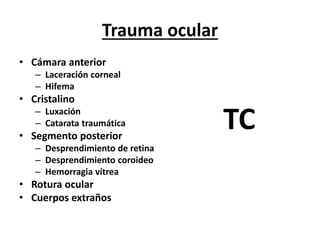
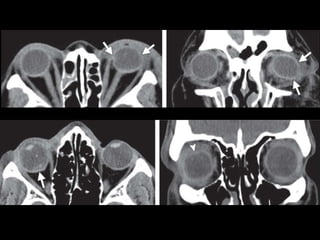
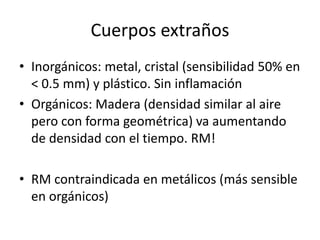
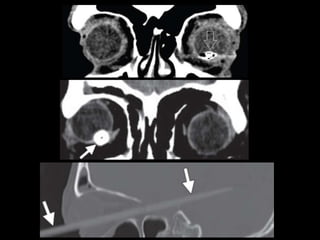
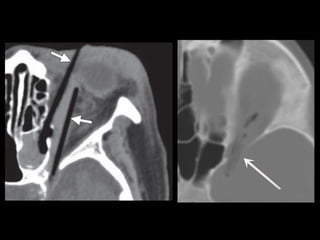
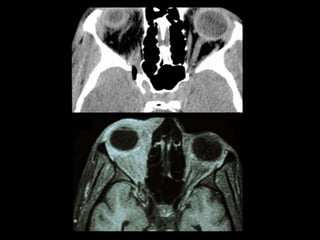
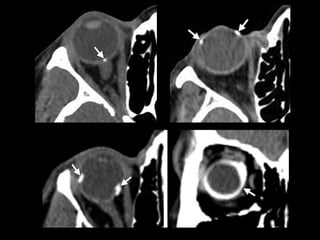
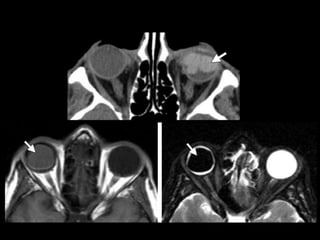
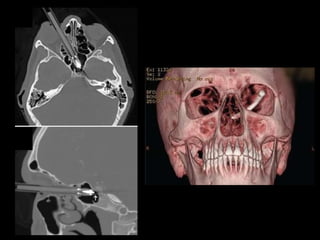

El documento trata sobre el trauma facial. Resume que la evaluación clínica incluye el manejo de la vía aérea, control de hemorragias y detección de lesiones asociadas como en la columna cervical. Explica las prioridades quirúrgicas y tipos de fracturas como las de Le Fort, naso-orbito-etmoidales y cigomático-maxilares. También cubre complicaciones como las orbitarias y oftalmológicas, así como el tratamiento de cuerpos extraños oculares.











































































































