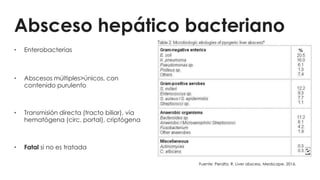
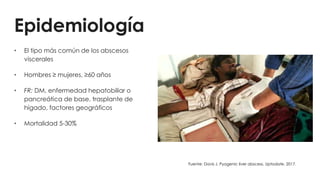
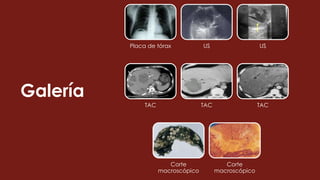
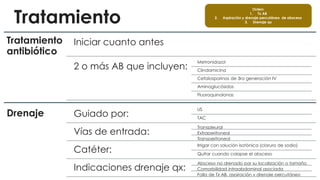
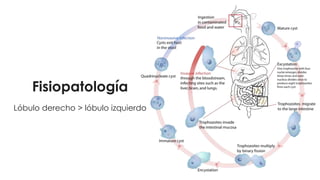
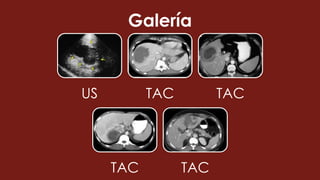
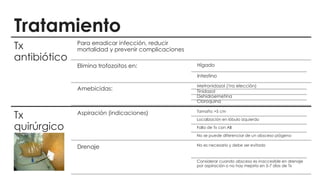
Este documento describe dos tipos principales de abscesos hepáticos: bacteriano y amebiano. El absceso hepático bacteriano es el más común, causado principalmente por bacterias entéricas y con mayor riesgo en personas con diabetes u otras enfermedades hepáticas. El absceso hepático amebiano es menos frecuente y causado por la Entamoeba histolytica, con mayor riesgo en viajeros a áreas endémicas. Ambos tipos se diagnostican mediante ultrasonido, TAC o resonancia magnética, y se tratan principal